Heart failure guidelines. A concise summary for the GP

Heart failure
Heart diseases
Guidelines have recently been released by the National Heart Foundation of Australia and the Cardiac Society of Australia and New Zealand on the prevention, detection and management of heart failure in Australia. This article provides a brief and practical summary of the guidelines, focusing on their application to diagnosis and management of heart failure in general practice.
- Heart failure (HF) is generally categorised as HF associated with a reduced left ventricular ejection fraction (LVEF) below 50% (HFrEF) or HF associated with a preserved LVEF of 50% or higher (HFpEF).
- Echocardiography is the single most useful investigation in patients with suspected HF. If not available in a timely fashion, measurement of plasma B-type natriuretic peptide (BNP) or N-terminal pro-BNP levels improves diagnostic accuracy.
- ACE inhibitors (or angiotensin receptor blockers [ARBs]), beta blockers and low-dose mineralocorticoid receptor antagonists (MRAs) improve survival and decrease hospitalisation in patients with HFrEF.
- The ACE inhibitor (or ARB) should be changed to an angiotensin receptor neprilysin inhibitor (unless contraindicated or not tolerated) for patients with HFrEF associated with an LVEF of 40% or less despite initial medical management.
- Ivabradine should be considered for patients with HFrEF associated with an LVEF of 35% or less and a sinus rate of 70 beats/min or greater despite standard medical management (including a beta blocker unless contraindicated).
- Referral for implantable cardioverter defibrillators and/or cardiac resynchronisation therapy should be considered for patients with persistent HFrEF associated with an LVEF of 35% or less despite optimal medical therapy.
- Low-dose MRAs may be considered to decrease HF hospitalisation in patients with HFpEF.
- Multidisciplinary HF disease management, nurse-led medication titration and exercise training have been shown to improve outcomes in patients with HF.
- Comorbidities should be identified and managed in all patients with HF.
- Referral to palliative care services should be considered in patients with advanced HF.
The National Heart Foundation of Australia and the Cardiac Society of Australia and New Zealand have recently released Guidelines for the prevention, detection and management of heart failure in Australia 2018.1,2 This article provides a concise and practical synopsis of the guidelines, with a focus on their application to diagnosis and management of patients with heart failure (HF) in general practice.
What is heart failure?
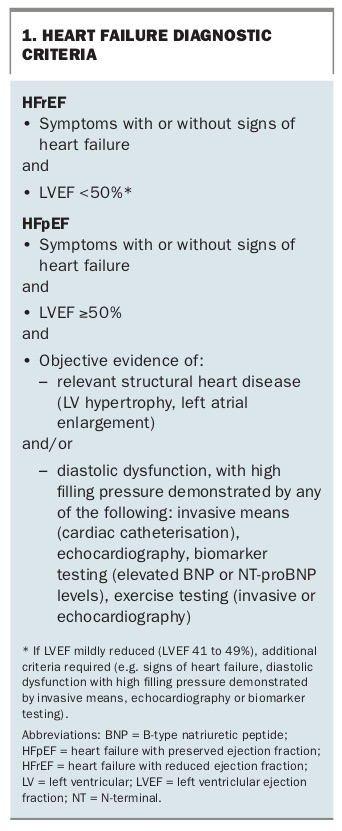
HF is a clinical syndrome with symptoms (usually dyspnoea) and signs secondary to an abnormality of cardiac structure or function that impairs the ability of the heart to fill with blood at normal pressure or eject blood sufficient to fulfil the needs of the metabolising organs. Once a clinical diagnosis of HF is made, it is generally classified according to the left ventricular ejection fraction (LVEF), into either HF associated with a reduced LVEF below 50% (HFrEF) or HF associated with a preserved LVEF of 50% or higher (HFpEF). This distinction is usually made with echocardiography. In patients with HFpEF or in those with HFrEF associated with only a mildly reduced LVEF (41 to 49%), additional diagnostic criteria are required (Box 1).
{kind=link}
Epidemiology of heart failure
HF affects over 38 million people worldwide and it is estimated that about 480,000 people in Australia are affected.3,4 HF is more common in the elderly, and the age-standardised prevalence of HF is 1.7-fold higher in Indigenous Australians compared with non-Indigenous Australians.5 The prevalence of HF is increasing at least in part due to the ageing population and better survival in patients with cardiovascular disease. Patients with HF experience repeated hospitalisations with overall survival worse than most non-haematological malignancies.6,7
Heart failure prevention
Although largely based on observational studies, smoking cessation, avoidance of excess alcohol, weight reduction (if overweight or obese) and regular physical activity are all strongly recommended to decrease the risk of developing HF.8-13 Pharmacological interventions that have been shown to decrease the risk of developing HF in large-scale, randomised controlled trials include use of blood pressure-lowering and lipid-lowering therapies, according to published guidelines, ACE inhibitors in patients with cardiovascular disease, and sodium glucose cotransporter-2 inhibitors in patients with type 2 diabetes associated with cardiovascular disease and insufficient glycaemic control despite first-line glucose-lowering therapy (usually metformin).14-17 ACE inhibitors and beta blockers are also strongly recommended in patients with asymptomatic left ventricular systolic dysfunction.18,19
Approach to diagnosis and monitoring of heart failure
HF is a clinical diagnosis that may be made following the initial history taking, physical examination and chest x-ray (Flowchart 1). Further initial investigations including a 12-lead electrocardiogram, blood biochemistry and full blood count should be performed to assess comorbidities and identify alternative causes of fluid overload. The echocardiogram is the single most useful investigation in patients with suspected HF. It improves diagnostic accuracy and provides additional structural and functional information (including measurement of LVEF and assessment of valvular function) to guide management. However, if the diagnosis is unclear and an echocardiogram cannot be arranged in a timely fashion, then measurement of plasma B-type natriuretic peptide (BNP) or N-terminal pro-BNP levels improves diagnostic accuracy.20
Further evaluation to determine the aetiology of HF is important. The need for specific imaging investigations to diagnose coronary artery disease such as invasive coronary angiography, CT coronary angiography, cardiac magnetic resonance imaging or stress imaging will be determined by the presence or absence of angina and the pre-test probability of coronary artery disease. Cardiac magnetic resonance imaging, positron emission tomography or bone scintigraphy may be performed in patients with HF associated with unexplained increased left ventricular wall thickness to diagnose inflammatory or infiltrative cardiomyopathies.
Clinical evaluation to identify symptoms or signs of congestion, serum biochemistry, full blood count and 12-lead electrocardiography should be performed regularly (six to 12 monthly once stabilised) and if there is a change in clinical status. The echocardiogram is usually repeated three to six months after commencing medical therapy in patients with HFrEF to guide further management, including the need for device therapy.
Management of acute heart failure
The management of acute HF should be guided by the patient’s vital signs, oxygen saturation and the presence or absence of congestion and hypoperfusion. Management includes use of intravenous diuretics in most patients accompanied by the selected use of oxygen therapy (if hypoxaemic), positive pressure ventilation, vasodilators and inotropes.2
Management of heart failure associated with a reduced LVEF
Several medical and device-related therapeutic interventions have been shown to improve survival, decrease HF hospitalisation and improve symptoms and quality of life in patients with HFrEF (Flowchart 2).
Initial medical management
ACE inhibitors, beta blockers and low-dose mineralocorticoid receptor antagonists (MRAs) have all been shown to improve survival and decrease hospitalisation in patients with HFrEF associated with a moderate or severe reduction in LVEF.21-27 These treatments are therefore strongly recommended in all patients with HFrEF associated with an LVEF of 40% or less unless contraindicated or not tolerated; and may also be considered in patients with HFrEF associated with an LVEF of 41 to 49%.28-30
An ACE inhibitor (or angiotensin receptor blocker [ARB] if an ACE inhibitor is contraindicated or not tolerated) is usually started initially (often in combination with a loop diuretic to manage congestion). A beta blocker (specifically bisoprolol, carvedilol, metoprolol controlled release or extended release, or nebivolol) is then added once the patient is stabilised with no or minimal clinical congestion on physical examination, either before or after the MRA (low-dose spironolactone or eplerenone 25 to 50 mg daily; Flowchart 2). These treatments are started at low doses and gradually uptitrated (usually doubled every two to four weeks) aiming for target doses.31 However, uptitration should not be to the detriment of starting other drugs that have been shown to decrease mortality in patients with HFrEF, with the aim to have the patient on a combination of all three classes of medical therapy, even if only low doses are able to be achieved.
Medications used in selected patients
Loop diuretics are favoured to manage congestion and are usually started at low doses, such as 20 to 40 mg furosemide orally daily.32 Ongoing monitoring of fluid status, electrolytes and renal function is important and the diuretic dose adjusted according to clinical response. Patients may also be educated to adjust the diuretic dose according to their symptoms and daily weight measurements. Thiazides or thiazide-like diuretics may be added to loop diuretics in patients with refractory congestion; however, close monitoring of electrolytes and renal function is required.
In patients with HFrEF associated with an LVEF of 40% or less despite initial medical management, the ACE inhibitor (or ARB) should be changed to a low or moderate dose of an angiotensin receptor neprilysin inhibitor (ARNI) (unless contraindicated or not tolerated) and gradually uptitrated every two to four weeks aiming for the target dose (see Flowchart 2).31 This recommendation is based on the Prospective Comparison of ARNI with ACEI to Determine Impact on Global Mortality and Morbidity in Heart Failure Trial (PARADIGM-HF) in which the ARNI (sacubitril-valsartan) was shown to improve survival and decrease hospitalisation compared with an ACE inhibitor (enalapril) in such patients.33 In view of an increased risk of angioedema, concomitant use of ACE inhibitors and ARNIs is contraindicated, and at least a 36-hour washout period should be allowed when switching therapy. ARNIs are generally well tolerated, but are associated with a higher incidence of hypotension, so are generally avoided or used cautiously if the systolic blood pressure is persistently below 100 mmHg.
Ivabradine should also be considered in patients with persistent HFrEF associated with an LVEF of 35% or less and a sinus rate of 70 beats/min or higher despite standard medical management (including a maximally tolerated or target dose of a beta blocker unless contraindicated); however, the approved indication of ivabradine in Australia requires a sinus rate of 77 beats/min or higher (Flowchart 2). This recommendation is based on the Systolic Heart failure treatment with the If Inhibitor Ivabradine Trial (SHIFT), in which ivabradine reduced cardiovascular mortality and HF hospitalisation, with greater benefit observed in patients with faster sinus rates.34 Ivabradine is a sinus node inhibitor and should therefore only be used in patients in sinus rhythm.
Additional treatment options used in very selected patients include hydralazine plus nitrates, N-3 polyunsaturated fatty acids and low-dose digoxin (aiming for serum digoxin levels of 0.5 to 0.9 ng/mL).35-39
Unless a reversible cause of HFrEF has been identified and corrected, neurohormonal modulators (ACE inhibitors, ARBs, ARNIs, beta blockers, MRAs) should be continued long-term even if the LVEF improves, to decrease the risk of recurrence.40,41
When to consider cardiac electronic device therapy
Implantable cardioverter defibrillators to treat malignant ventricular arrhythmias and cardiac resynchronisation therapy to allow biventricular pacing to resynchronise ventricular contraction in patients with a broad QRS (130 ms or more) have been shown to improve outcomes in selected patients with persistent HFrEF associated with a moderate or severe reduction in LVEF (LVEF of 35% or less) despite optimal medical therapy.42-45 Such patients should be reviewed by a cardiologist to consider whether these treatments should be offered.
Surgical and percutaneous management of coronary artery disease and valvular heart disease
Patient selection and procedural planning for the surgical or percutaneous management of coronary artery disease and valvular heart disease in patients with HF is guided by a multidisciplinary heart team. The long-term clinical benefits need to be balanced against the short-term morbidity and mortality associated with these procedures, with additional considerations including the presence of associated comorbidities and patient frailty. Coronary artery bypass surgery or percutaneous coronary intervention may be undertaken in patients with haemodynamically significant coronary artery stenoses, even if associated with a moderate or severe reduction in LVEF (LVEF of 35% or less), with the evidence for improved clinical outcomes being strongest for coronary artery bypass surgery.46
Surgical aortic valve replacement is recommended in patients with HF associated with either severe aortic stenosis or severe aortic regurgitation in the absence of major comorbidity or frailty to improve symptoms and survival.47 Alternatively, transcatheter aortic valve implantation may be undertaken in selected patients with HF and severe aortic stenosis who are considered inoperable or at intermediate to high risk of operative mortality for surgical aortic valve replacement.48-51 Surgical mitral valve repair or replacement may be undertaken in patients with HF associated with moderate- to-severe mitral regurgitation at the time of elective coronary artery bypass surgery.52 The role of surgical or percutaneous mitral valve repair or replacement in patients with HF associated with severe functional mitral regurgitation despite optimal medical and device therapy is evolving.53,54
Ventricular assist device therapy and heart transplantation
Patients with intractable, severe HF despite optimal medical therapy and pacemaker therapy (if indicated) have a particularly poor prognosis. In the absence of major comorbidities, such patients should be referred to specialist HF centres, to consider further treatment options including ventricular assist device therapy and heart transplantation.55,56
Management of heart failure associated with a preserved LVEF
According to registry studies, HFpEF accounts for about one-half of all cases of HF.57 These patients are usually elderly with multiple comorbidities. In contrast to the rich evidence-base in HFrEF, none of the large-scale randomised controlled trials conducted to date in patients with HFpEF have achieved their primary endpoint.58-61 However, there have been reductions in HF hospitalisation observed in some studies evaluating MRAs and ARBs.58,61 Loop diuretics are usually required to manage congestion (although thiazide or thiazide-like diuretics may be preferred in patients with predominant hypertension). Comorbidities, including hypertension, ischaemic heart disease, diabetes and atrial fibrillation, should be identified and managed. Low-dose MRAs may be considered to decrease HF hospitalisation.61
Models of care to improve evidence-based practice
The most vulnerable period for patients with HF is within the first few weeks following discharge from hospital. These patients should be reviewed within one to two weeks, regardless of the type of appointment, to review and uptitrate medication. Patient and carer education about HF and self-management should be commenced soon after diagnosis, with ongoing revision. Several nonpharmacological strategies have been shown to improve evidence-based practice and patient outcomes in patients with HF, including multidisciplinary HF disease management, nurse-led medication titration and exercise training.
Multidisciplinary heart failure disease management
Multidisciplinary HF disease management refers to several interventions delivered by HF nurses in collaboration with cardiologists or specialist physicians, GPs, pharmacists, physiotherapists, occupational therapists, exercise physiologists, dietitians, psychologists and palliative care physicians, as appropriate. These models of care have been shown to improve survival and decrease rehospitalisations, especially in high-risk patients such as those recently admitted to hospital with HF.62 Although the evidence is strongest for face-to-face visits (either at home or in a clinic setting), if access to such care is limited, multidisciplinary telemonitoring or telephone-support programs have also been shown to improve outcomes.63,64
Nurse-led medication titration
Numerous registries have reported under-dosing of evidenced-based treatment in HF. Nurse-led medication titration has been shown to increase the proportion of patients achieving target doses of their medications, which translates into clinical benefits including decreased rehospitalisation and improved survival.65
Exercise training
Regular performance of up to moderate-intensity continuous exercise is recommended in patients with chronic HF, particularly in those with reduced LVEF, to improve quality of life and reduce hospitalisation for heart failure.66
Comorbidities
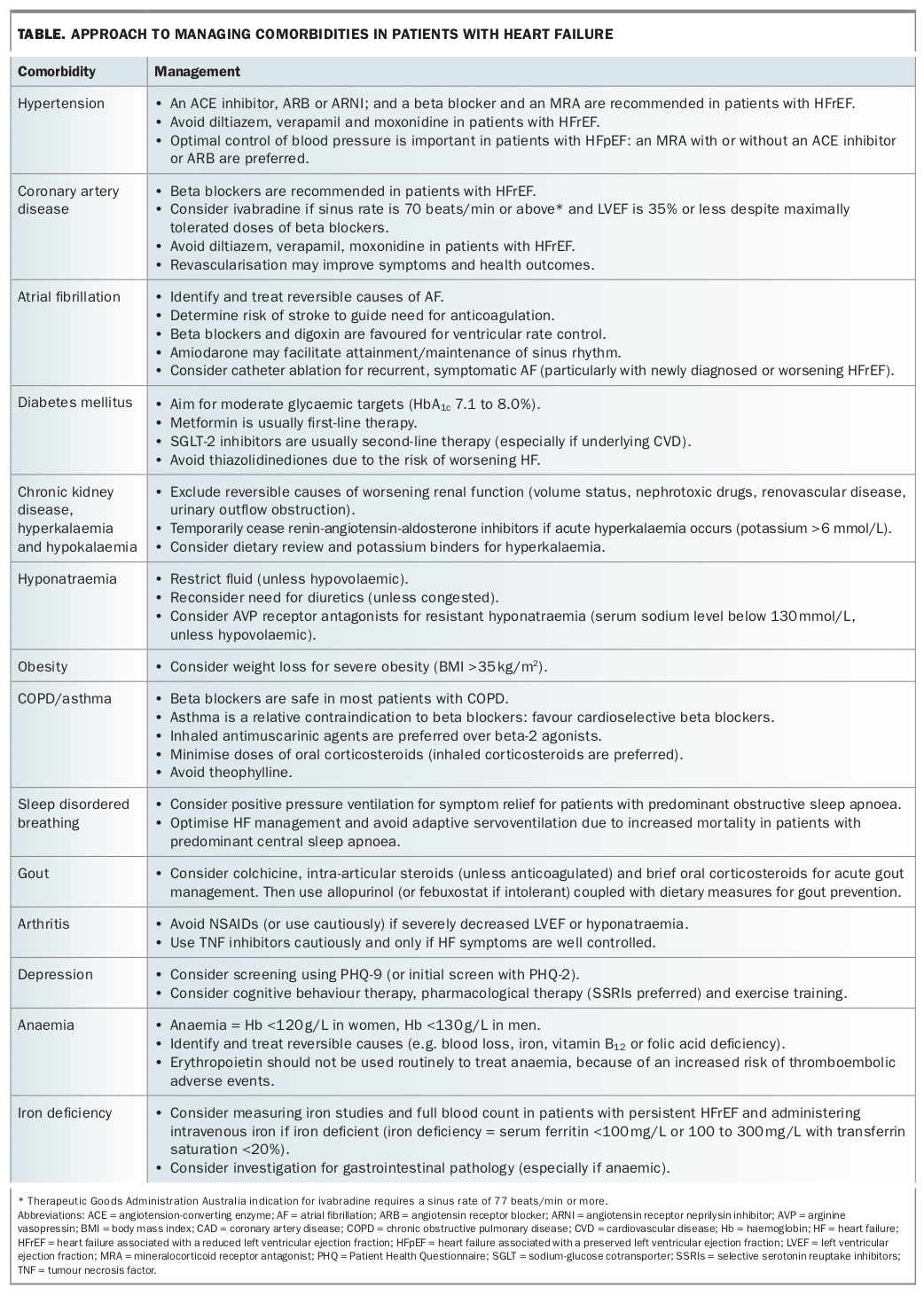
Comorbidities are common in patients with HF, are associated with worse quality of life and health outcomes, and may interfere with standard HF management. A structured framework to identify and address comorbidities has been proposed.67 A summary of the approach to managing comorbidities in patients with HF is provided in the Table.
{kind=link}
Palliative care
Palliative care services have been shown to alleviate end-stage symptoms, improve quality of life and decrease rehospitalisation.68 Referral to such services should be considered in patients with advanced HF, and should include discussions regarding ‘ceiling of care’ and deactivation of implantable cardioverter defibrillators. Patients with HF should be encouraged to have an advanced care plan.
How to measure quality of care in heart failure
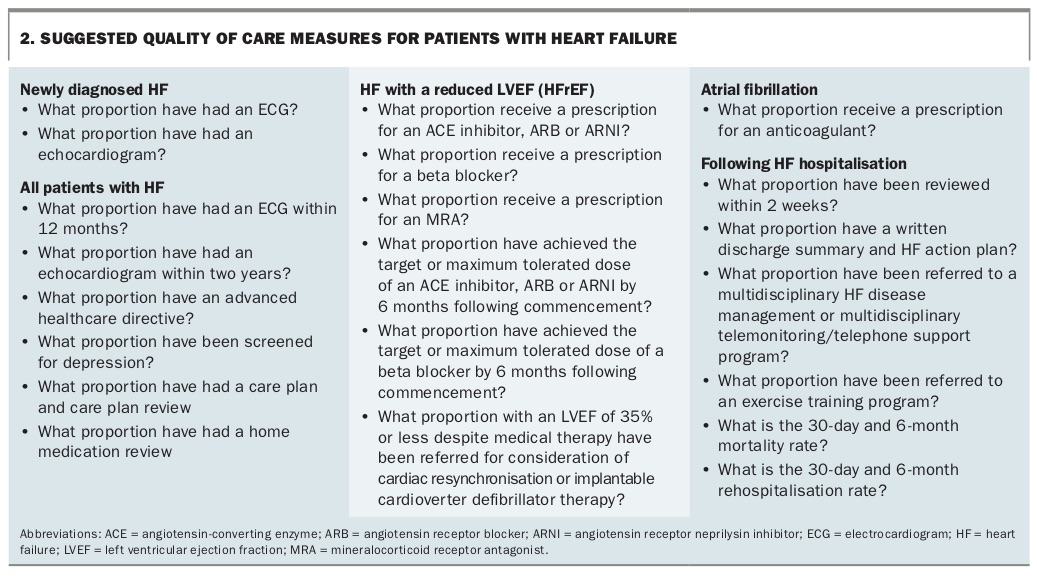
Better adherence to clinical guidelines is associated with better health outcomes. Ongoing audit and timely feedback should ideally be integrated into work practice to improve and maintain the quality of care. A list of suggested process and outcome quality measures is provided in Box 2.
{kind=link}
Conclusion
The HF guidelines are designed to facilitate the systematic integration of recommendations into the care of patients with HF. This includes ongoing audit and feedback systems integrated into work practices to improve the quality of care and outcomes of patients with HF. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.