Diagnosis of heart failure

Heart failure
Heart diseases
Heart failure is a complex clinical syndrome that presents a difficult diagnostic challenge for practitioners. Index of suspicion for heart failure and a clear understanding of the condition are crucial for timely and correct diagnosis and prompt provision of effective treatment.
- Heart failure (HF) is categorised as HF with reduced ejection fraction (formerly known as systolic HF) or HF with preserved ejection fraction (formerly known as diastolic HF).
- HF is diagnosed clinically but needs to be confirmed with further testing.
- Correct and timely diagnosis is important, as prompt treatment can save lives and improve quality of life.
- An echocardiogram is the most important investigation in HF; it will confirm the diagnosis and inform further management strategies.
- In patients for whom the diagnosis is unclear, biomarker analysis with B-type natriuretic peptide (BNP) or N-terminal pro-BNP can be useful.
The initial diagnosis of heart failure (HF) in a patient often presents a clinical challenge to the clinician. The experiences of patients, relatives and clinicians are littered with examples of delayed or incorrect diagnoses. This mainly reflects the complexity of the syndrome and its clinical manifestations, but also the syndrome’s unexpected occurrence in patients intuitively considered to be at low risk. Early symptoms and signs of HF can also mimic many other common conditions, which can often lead to a delay in diagnosis.
The consequences of late or incorrect diagnosis are clear, with patients suffering because of delayed provision of effective treatment or being at risk of adverse effects of unwarranted therapy (without benefit) if they have been misdiagnosed.
Index of suspicion for HF, as well as a clear understanding of the condition, is crucial for timely and correct diagnosis. Being aware of groups in whom HF is more common, such as people with previous myocardial infarction, longstanding hypertension or diabetes, and older people, is also crucial to ensuring adequate surveillance and early investigation.
This article focuses on the initial diagnosis of HF using guidance from the recently published National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand HF guidelines.1
Definition of heart failure
HF is defined as ‘a complex clinical syndrome with typical symptoms and signs that generally occur on exertion, but can also occur at rest (particularly when recumbent). It is secondary to an abnormality of cardiac structure or function that impairs the ability of the heart to fill with blood at normal pressure or eject blood sufficient to fulfil the needs of the metabolising organs’.1
This definition, like the disease itself, is complex. It warrants expansion of the many key concepts related to HF that it incorporates.
Complex clinical syndrome
The clinical complexity of the syndrome reflects the impact of cardiac dysfunction on many organ systems.
Typical symptoms and signs
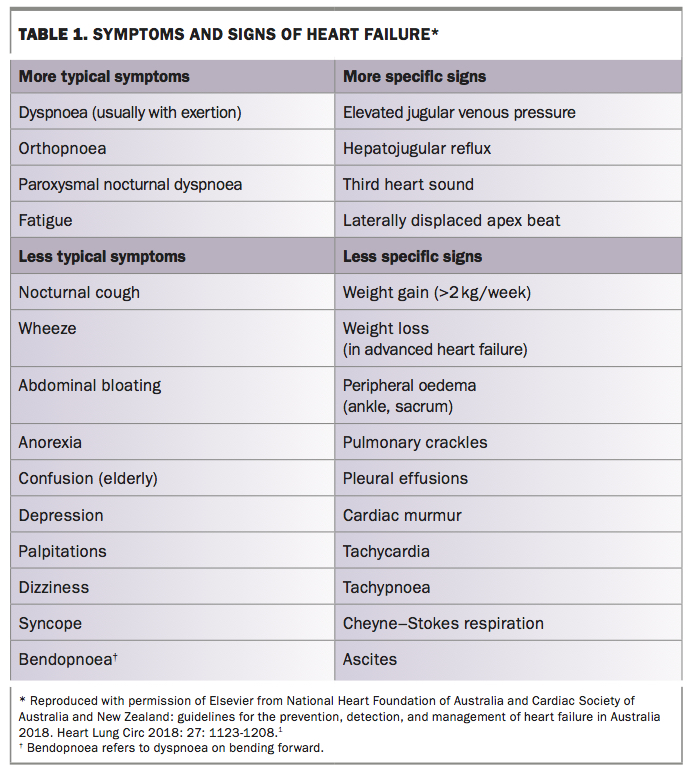
HF has typical symptoms, although they are often nonspecific. Dyspnoea is the cardinal symptom of HF but is especially nonspecific. However, some patterns of dyspnoea, such as orthopnoea, paroxysmal nocturnal dyspnoea and (to a lesser degree) exertional dyspnoea, are typical of HF. Other important HF symptoms are fatigue, peripheral oedema and occasionally solitary or dominant gastro-intestinal symptoms (e.g. abdominal bloating or discomfort and anorexia), reflecting right HF.
Typical signs of HF can be divided into those related to cardiac dysfunction and strain (tachycardia, third heart sound, murmurs and displaced apex beat); reduced end-organ perfusion; or congestion (abnormal cardiac filling resulting in high venous pressure), such as elevated jugular venous pressure, hepatic enlargement and tenderness, peripheral oedema, pulmonary crackles, pleural effusions and ascites (Table 1).
{kind=link}
On exertion, at rest and when recumbent
Symptoms of HF generally, and initially, manifest with physical exertion. As the syndrome progresses, symptoms occur at lower levels of physical activity and even at rest. The fluid shift that occurs during recumbency accounts for orthopnoea and paroxysmal nocturnal dyspnoea.
Abnormality of cardiac structure or function
Despite the end-organ impact of HF, the underlying problem is usually cardiac, most often involving ventricular myocardial systolic or diastolic dysfunction, or both. However, structural abnormalities of almost any cardiac component (from the valves to the pericardium, endocardium and conduction system) can lead to the HF syndrome.
Impaired ability of the heart to fill with blood at normal pressure
In diastole, the ventricle fills with blood. When the ventricle is unable to fill with blood without increased filling pressure (usually because of reduced ventricular compliance or active relaxation, or both), symptoms and signs of congestion of the vasculature and end organs will result.
Impaired ability of the heart to eject sufficient blood
If the heart is regarded as a pump, a reduction in ejection of blood to the extent that it is insufficient for the metabolising needs of the tissues will result in symptoms and signs.
Classification of heart failure by ejection fraction
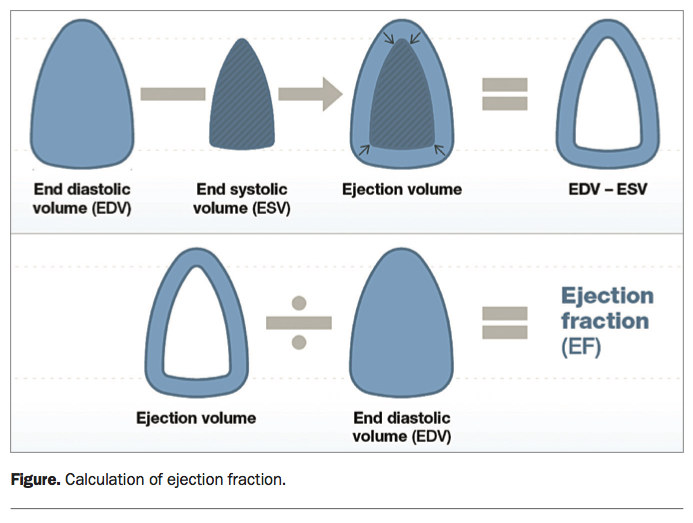
HF is diagnosed clinically. Patients diagnosed with HF may then be classified according to their left ventricular ejection fraction (LVEF). This well-established haemodynamic term reflects the percentage of ventricular volume that is ejected per heartbeat according to the equation:
EF = (EDV – ESV) ÷ EDV
where EF = ejection fraction (expressed as a percentage), EDV = end diastolic volume and ESV = end systolic volume (Figure).
{kind=link}
It follows that EF is a measure of cardiac ejection and therefore of systolic function. This haemodynamic parameter is central to the modern classification of HF syndromes. The lower limit of normal for LVEF is 50 to 55%. The subclassification based on LVEF is particularly important as it guides effective therapy.
Heart failure with reduced ejection fraction
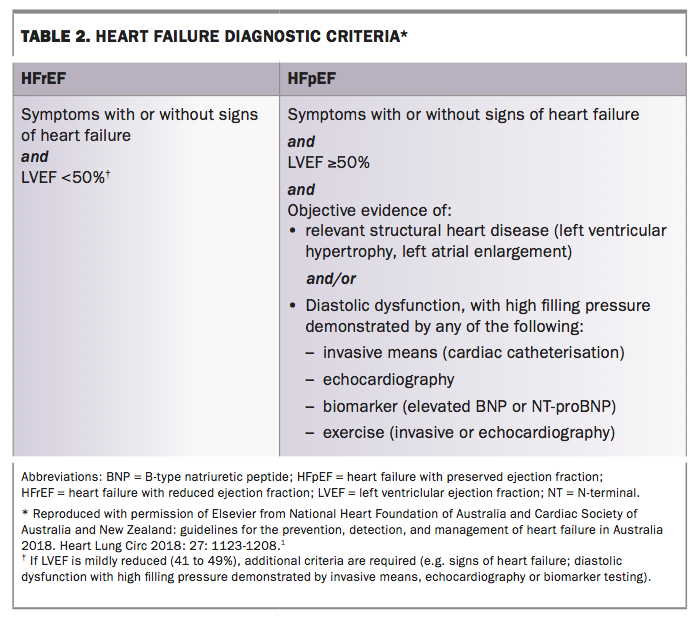
Heart failure with reduced ejection fraction (HFrEF), formerly known as systolic HF, is defined as having clinical symptoms with or without signs of HF and a measured LVEF of less than 50% (Table 2).
{kind=link}
Heart failure with preserved ejection fraction
Heart failure with preserved ejection fraction (HFpEF), formerly known as diastolic HF, has proven more difficult to define because LVEF, the key objective marker of cardiac abnormality, is, by definition, preserved. This leaves only the largely nonspecific clinical symptoms and signs. The definition of HFpEF therefore remains an evolving and dynamic concept, but it includes all of the following:
- clinical symptoms with or without signs of HF
- a measured LVEF of at least 50%
- objective evidence of either relevant structural heart disease or diastolic dysfunction showing increased filling pressure (Table 2).
Relevant structural heart disease refers to left ventricular hypertrophy or left atrial enlargement. Left ventricular hypertrophy reduces ventricular compliance. It is a common associated feature and potential cause of diastolic dysfunction, which results in high left-sided filling pressure. Left atrial enlargement is a consequence of high left-sided filling pressure.
Diastolic function incorporates two components: left ventricular compliance and active ventricular relaxation. Reduced ventricular compliance and abnormal ventricular relaxation may both result in increased left-sided filling pressure. Diastolic dysfunction therefore refers to documentation of high left-sided filling pressure, which can be done by invasive means, echocardiography or biomarker analysis.
The invasive approach requires a right heart catheter study with or without a left heart catheter study (performed by a cardiologist) to document raised pulmonary capillary wedge pressure (greater than or equal to 15 mmHg) or left ventricular end diastolic pressure (greater than or equal to 16 mmHg).
Data on cardiac filling pressure are generally always present on a standard echocardiogram. However, interpretation of the results, and specifically whether they suggest elevated left-sided filling pressure, is difficult and frequently unclear. Moreover, a summary statement (on filling pressure) by the reporting cardiologist is often lacking. One obvious user-friendly way to avoid not receiving the desired information on diastolic dysfunction and filling pressure in the final report is to specifically ask for it on the request form (e.g. ‘?HF, ?elevated filling pressure, ?diastolic dysfunction’).
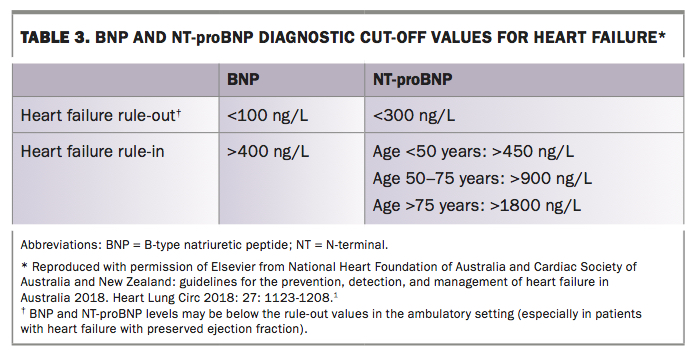
Biomarker analysis refers to using rule-in cut-off levels for natriuretic peptides (Table 3). B-type natriuretic peptide (BNP) and its N-terminal fragment (NT-proBNP) are endogenous peptides released from the ventricular myocardium in response to wall stress (i.e. elevated intracardiac filling pressure). They have been well validated as powerful and reliable markers of HF severity and prognosis and consequently have a role in diagnosis. Their usefulness is somewhat attenuated in HFpEF, where levels are not as consistently elevated as in HFrEF, and also by variability in levels relating to age, renal function, female sex (elevated) and obesity (reduced). Further, the cost of the test ($40 to $80) in clinical practice outside the emergency setting in Australia falls to the patient, due to reimbursement restrictions. These riders by no means overwhelm the usefulness of this underused test in the diagnosis of HF in Australia.
{kind=link}
Left ventricular ejection fraction cut-off
The ability to classify HF when the LVEF is 40 to 50% has long been a source of controversy among cardiologists and, therefore, confusion for treating practitioners. The new guidelines tried to resolve this by choosing a 50% LVEF cut-off to differentiate between HFrEF and HFpEF.1
It is recommended that, in the setting of clinical symptoms with or without signs of HF, an LVEF of 50% or more be considered HFpEF and an LVEF of less than 50% be considered HFrEF, to inform management strategy.
HFrEF where the LVEF has improved to more than 50% with treatment (so-called recovered HFrEF) should generally be considered and treated the same as HFrEF because the pathophysiology is not believed to have changed. Indeed, recent data strongly suggest significant recurrence rates when prognostic therapy is ceased in patients with recovered HFrEF.2
Demography of heart failure
Heart failure with reduced ejection fraction
In Australia, HFrEF is most often secondary to ischaemic heart disease (about 50 to 60% of cases). Other common causes include toxic cardiomyopathy (e.g. prolonged excessive consumption of alcohol, illicit misuse of stimulant drugs, chemotherapy agents), genetic cardiomyopathy, inflammatory cardiomyopathy, uncontrolled tachyarrhythmias and idiopathic cardiomyopathy (Box).1
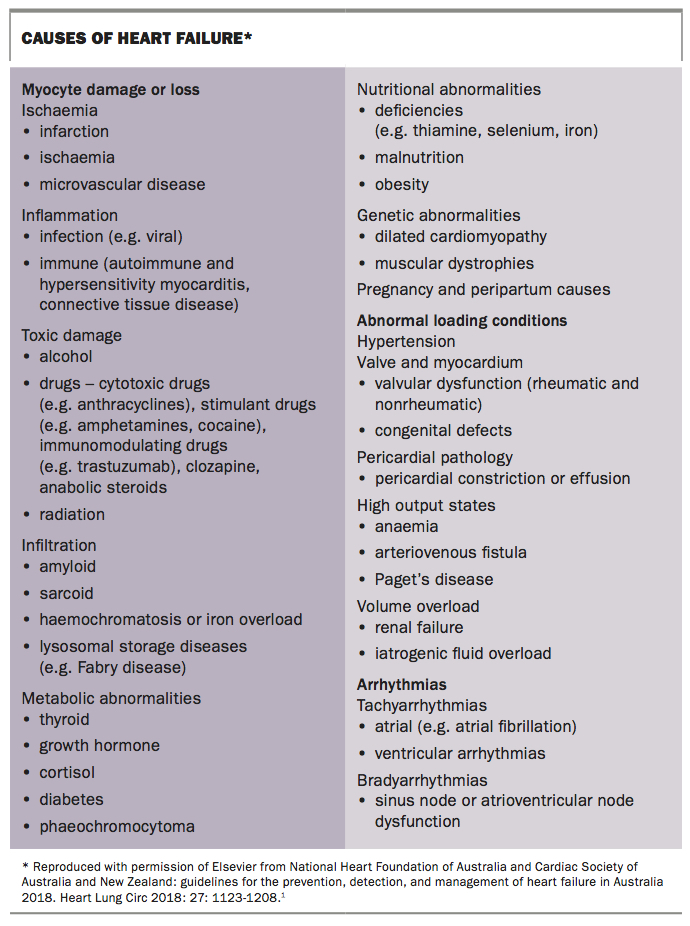{kind=link}
Heart failure with preserved ejection fraction
HFpEF makes up about half of HF cases. It is predominantly a syndrome of the elderly and more often occurs in women. Typical comorbidities associated with HFpEF are obesity, diabetes, hypertension and atrial fibrillation.1
Clinical workup for diagnosis
As HF most often represents an insidious syndrome with a slowly progressive decline in clinical status, its possibility as a diagnosis is often overlooked. The importance of clinical suspicion for a new diagnosis of HF as the cause of a patient’s presentation cannot be overstated. Once the potential diagnosis is brought to the front of the practitioner’s mind, history and examination tailored towards diagnosing HF (as in Table 1) naturally follow.
Initial investigations in HF diagnostic workup aim to:
- exclude other diagnoses
- assist with confirmation of HF diagnosis
- allow HF characterisation (HFrEF or HFpEF)
- define the cause of HF.
From the perspective of investigations that are readily available in primary care, these can be divided into blood tests, imaging studies, basic cardiac investigations and basic respiratory investigations. Table 4 lists useful initial investigations with general (albeit variable) availability to the diagnosing practitioner and characterises what type of information they provide in relation to the above aims.
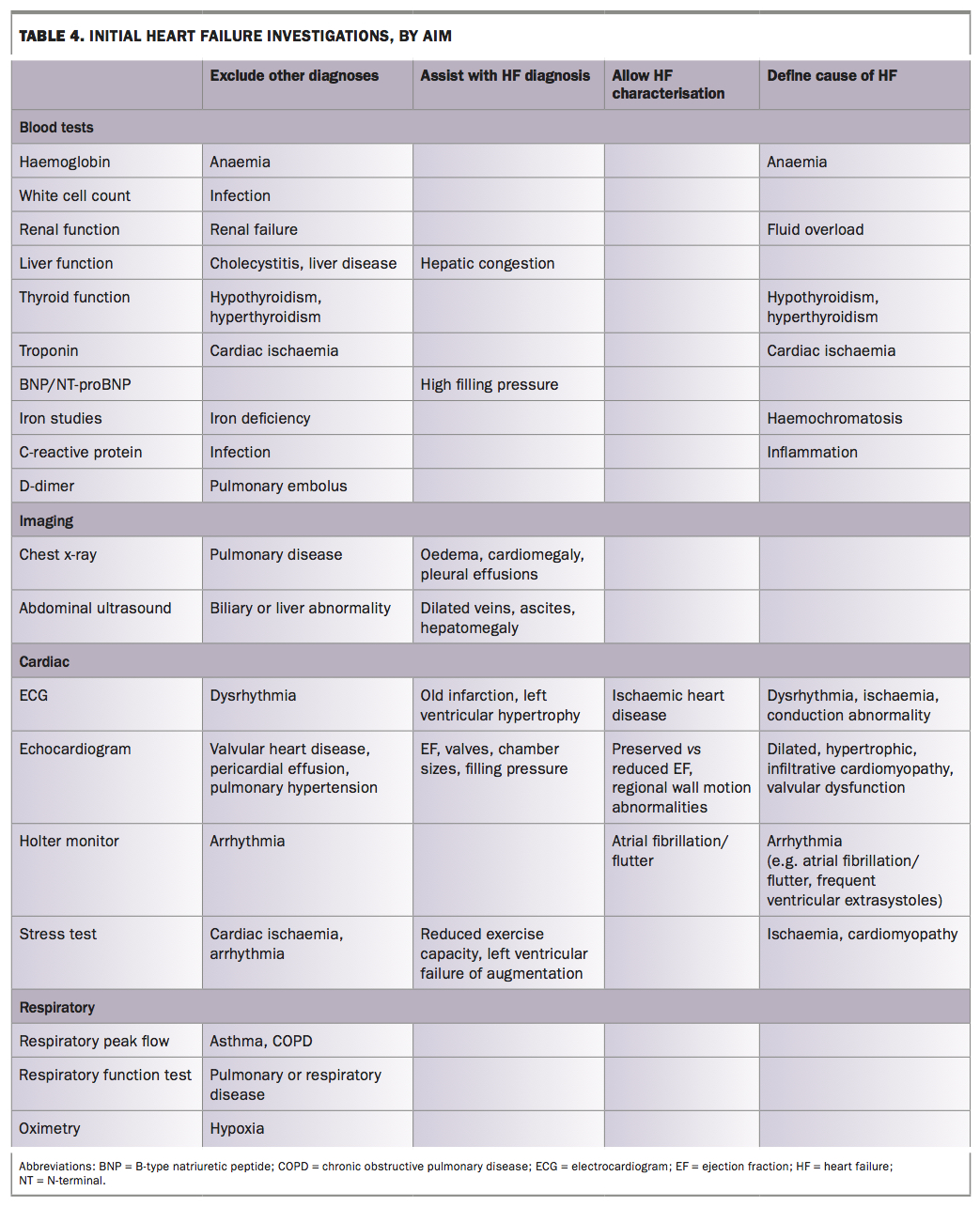{kind=link}
Once a clinical suspicion of HF exists, the Flowchart (see Heart failure guidelines, page 5) should be followed to determine the presence or absence of HF. An echocardiogram is the most important investigation in HF, as it will confirm the diagnosis and inform further management strategies. Therefore, when a clinical diagnosis is made, or there is strong suspicion of HF, an echocardiogram is organised. When there is uncertainty, either an echocardiogram or BNP/NT-proBNP measurement can be used. BNP/NT-proBNP levels can also be used to confirm clinical suspicion if an echocardiogram is not available in a timely manner. If alternative diagnoses have been pursued initially, but there is still doubt about the ultimate diagnosis, tests for HF – either echocardiography or BNP/NT-proBNP – may be useful.
If HF is not confirmed, other causes should be investigated. Many people will have comorbid conditions, such as chronic obstructive pulmonary disease, in addition to HF. However, HF should not be ruled out based only on a history of other conditions. It is imperative to actively exclude HF in these situations.
Conclusion
HF is a serious condition that has a very poor outcome. Early diagnosis and intervention are key to reducing morbidity and mortality for patients with HF. As HF is often undiagnosed, a high index of suspicion is imperative for early diagnosis. The diagnosis itself can be difficult, as it requires a combination of clinical and investigative processes, and the disease entity has two distinct forms: HFrEF and HFpEF. Correct and timely diagnosis has clear rewards, as it allows the provision of life-saving treatments that can improve quality of life and alter the natural history of the disease. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.