What's new in weight loss management and surgery?


Obesity
Weight loss surgery
Managing obesity is challenging and new treatment involves multimodal long-term care tailored to each patient. Dietary and lifestyle management are cornerstone to all treatment options, and pharmacotherapy has an adjuvant role in aiding appetite suppression. In people with morbid obesity and those with obesity and comorbidities, durable weight loss can be safely achieved with bariatric surgery. There are several surgical options, with current evidence favouring sleeve gastrectomy.
Obesity: a rising burden of disease in current times
Obesity, defined as abnormal or excessive fat accumulation that may impair health, is a polymorphic chronic disease that has increased in both incidence and prevalence throughout the 20th and 21st centuries.1 It has reached epidemic proportions and is now one of the most important public health issues globally.2 During the COVID-19 pandemic, it also appears that people with obesity have been disproportionately affected.3 The risk of coronavirus-related hospital death increases 1.5 to two times for people with a body mass index (BMI) of 30 kg/m2 to more than two times for those with a BMI of 40 kg/m2 or more.
The most commonly used criterion for obesity is a BMI of 30 kg/m2 or more. However, BMI should be used as a crude measurement, keeping in mind that certain groups in the Australian population, such as people of South Asian descent, are prone to the complications of obesity at lower BMIs.4
Body weight and fat mass are highly heritable traits, with important genetic and epigenetic aetiological factors.5 The rise in the prevalence of obesity has largely been driven by environmental factors including an abundance of calorie-rich food and a lack of physical activity.6 Based on World Health Organization data, an estimated 650 million adults worldwide were obese in 2016 and 2.1 billion were overweight.7 It is predicted that without significant action approximately 223 million children will have excess weight by 2025.7,8
The incidence of comorbidities that have obesity as a strong contributory factor and are responsible for a large public health burden have risen along with those of obesity. These comorbidities include type 2 diabetes, cardiovascular disease (e.g. coronary heart disease, cerebrovascular disease), musculoskeletal disorders (e.g. osteoarthritis) and cancers with an aetiological association with obesity (e.g. oesophageal adenocarcinoma and some breast, ovarian, prostate, liver, colon and renal cancers).9
The challenge of treating obesity requires a commitment from the patient to lifelong permanent changes in eating and activity behaviours. Achieving this involves combinations of low-calorie diets, exercise programs, pharmacotherapy and, in some patients, bariatric surgery.
Medical therapy
Doctors should be familiar with the basic principles of pharmacotherapy for obesity. For more than 20 years, the US National Institutes of Health has recommended that individuals who fail to respond to lifestyle interventions after six months of treatment, and have a BMI of 30 kg/m2 or more, or a BMI of 27 kg/m2 or more with weight-associated comorbidities, may be considered for weight loss medication treatment.10
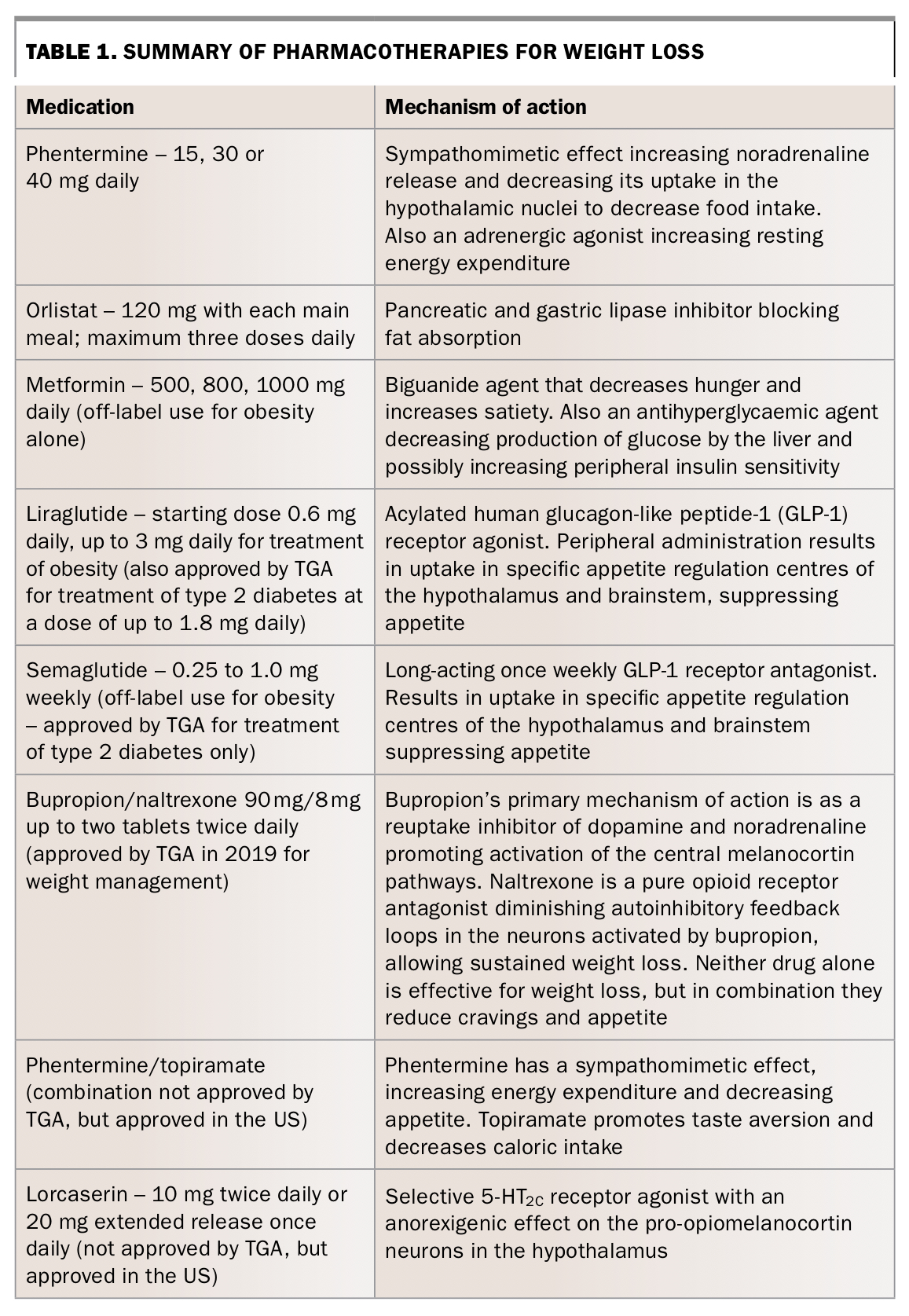
Pharmacotherapy has an adjuvant role to diet and exercise and may be helpful to ‘kick start’ weight loss and aid appetite suppression. Pharmacotherapy adjuncts for weight loss date back to the 1920s, and agents such as phentermine have been used since the 1950s.11 Newer formulations offer greater flexibility of dosing and there are now new combinations of drugs, some of which have recently been made available in Australia.
Liraglutide, which was first used to treat type 2 diabetes, centrally exploits the hypothalamic target for appetite suppression and delay gastric emptying. Semaglutide is a genetically engineered glucagon-like peptide-1 receptor agonist, which has shown sustained glycaemic control and weight loss benefits in trials.12,13 As a peptide, it has to be given as a weekly subcutaneous injection. It is available on the PBS for the treatment of type 2 diabetes but it is not approved by the TGA or subsidised on the PBS for weight loss.
Combination therapies include phentermine and topiramate (combination not approved for use in Australia), which combines a weight loss drug with an antiepileptic drug for a greater weight loss effect, but tolerability limits its use.14 Buproprion/naltrexone therapy combines naltrexone HCl, which is more commonly used to treat substance abuse conditions, and bupropion HCl, which is an antidepressant. These two medications work together in the brain to help downregulate hunger signalling.
Pharmacotherapies used in weight loss management and their mechanisms of action are listed in Table 1. Patient responses to these therapies vary for clinically meaningful weight loss (more than 5% body weight loss after 12 weeks of therapy).
{kind=link}
Surgical intervention
At a patient management and therapeutic level, bariatric surgery (also known as weight loss surgery) is increasingly being relied on as the most effective way to enable significant durable weight loss in patients with severe obesity who fail to respond to genuine efforts with dietary, exercise and lifestyle measures. The 2011 review of surgical interventions for the treatment of obesity from the Australian Government Department of Health supports this approach.15 The new term ‘metabolic surgery’ recognises the physiological benefits of these procedures (chief among them, reversal of diabetes risk).16
Bariatric operations have traditionally been categorised according to the mechanism by which weight loss ensues as:
- restrictive procedures (limit intake)
- malabsorptive procedures (interfere with digestion and absorption)
- combination of the above procedures.
Selection of patients for bariatric surgery
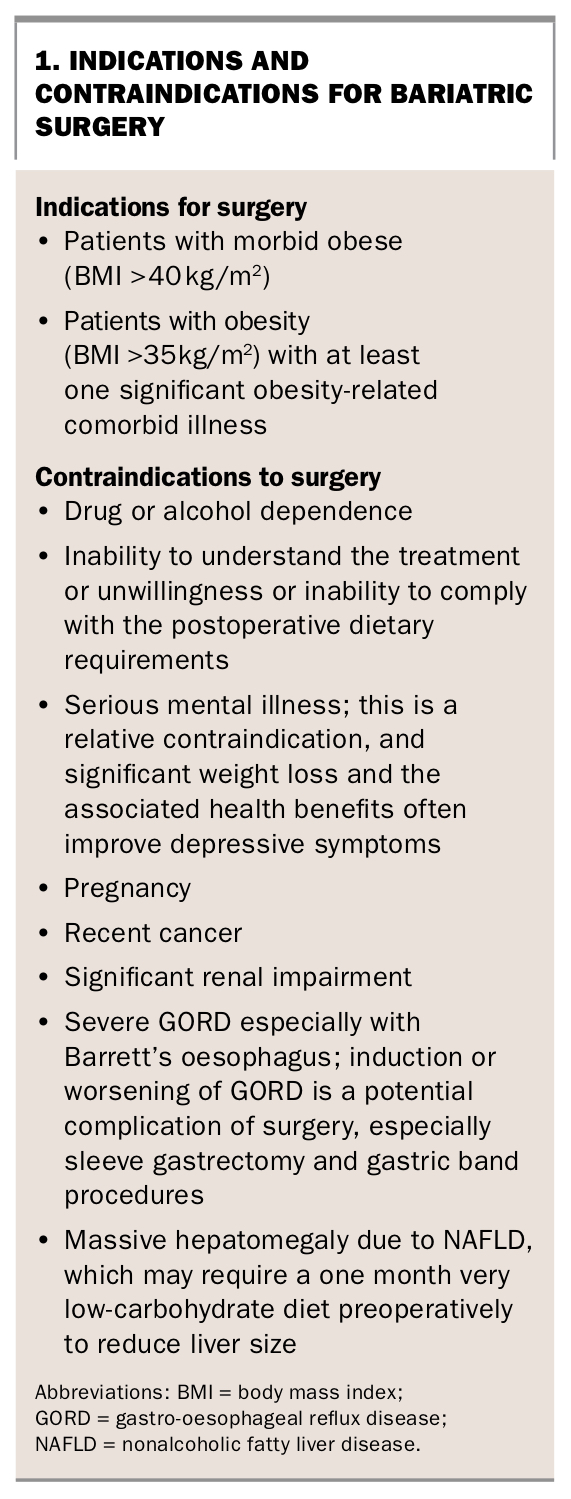
Although some patients with obesity have success with early intervention and modifications to diet and lifestyle, many are unable to achieve adequate sustained weight loss. The National Health and Medical Research Council guidelines state that people with obesity can be selected for bariatric surgery if they have failed sustained efforts with dietary and lifestyle therapies.17 Bariatric surgery should be discussed with motivated patients who have a BMI of 35 kg/m2 or greater and one or more obesity-associated comorbidities. Reflecting the low success rates with nonsurgical approaches, bariatric surgery can also be considered in patients with morbid obesity (BMI of 40 kg/m2 or more) even in the apparent absence of obesity-related comorbid disease. The indications and contraindications for bariatric surgery are listed in Box 1.
{kind=link}
The GP’s role
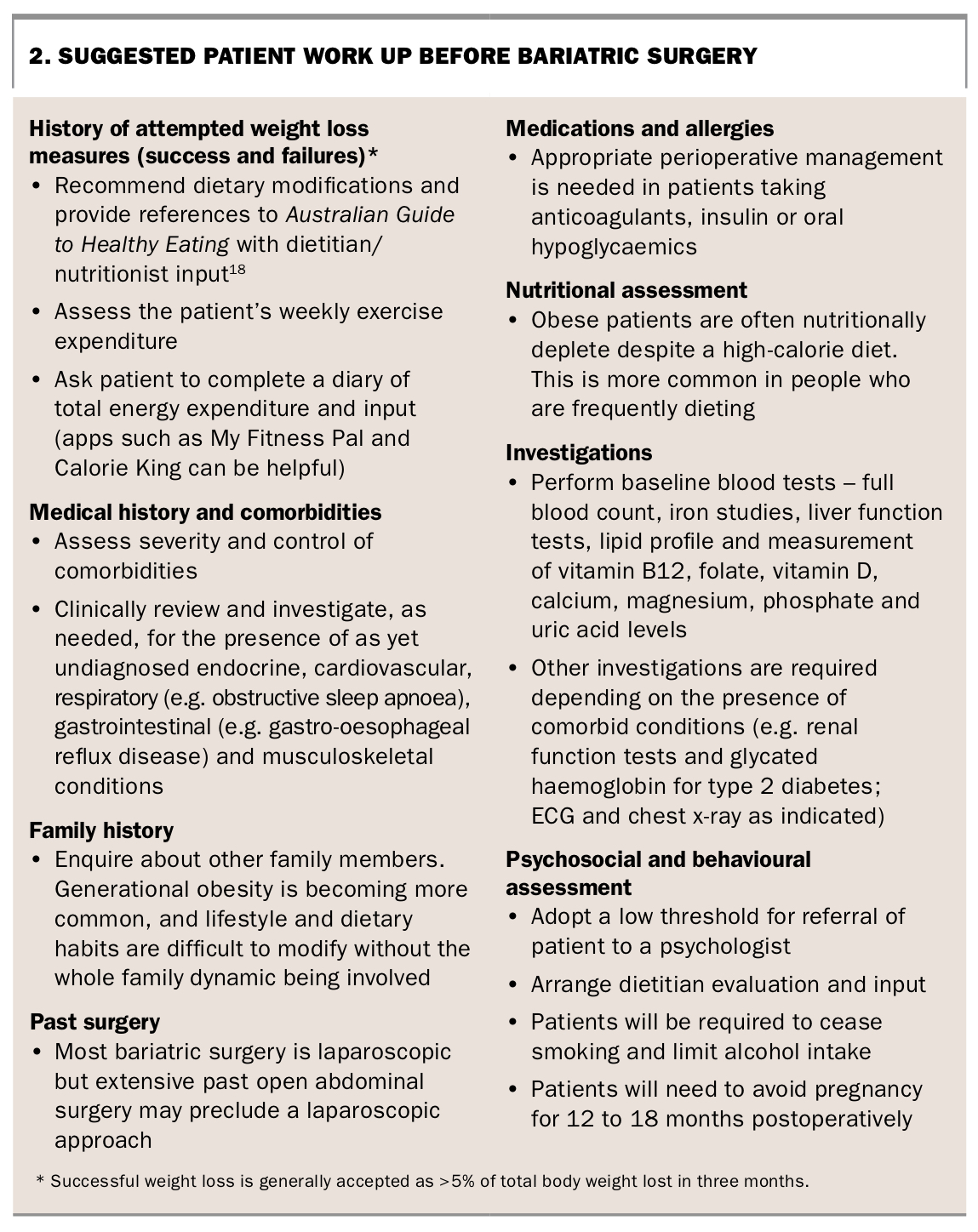
Work up for patients with obesity who are considering bariatric surgery is important (Box 2).18 This is often performed by the GP although patients are increasingly being referred to an endocrinologist with an interest in obesity treatment, a surgeon who performs bariatric surgery or a multidisciplinary clinic with specialist physician, surgeon, dietitian, exercise physiologist and psychologist expertise available.
{kind=link}
Failed dietary and lifestyle management is the impetus for surgical referral. It is accepted that three to six months of lifestyle change be trialled before putting patients forward as candidates for surgical management. During this time, the patient’s level of motivation to adopt major lifestyle changes can be assessed. A realistic and sustainable diet plan should be implemented rather than a ‘fad’ diet. Pharmacotherapy adjuncts should be used, taking into consideration other obesity comorbidities and intercurrent health management issues.
Patients may seek advice from their GP regarding suitability, operation selection and risk of complications. They have often discussed the procedure with others who have undergone weight loss surgery and many have also performed online research. Patients need to be made aware that there is not yet medium or long-term evidence to support some novel techniques such as some endoscopic procedures. An outline of the different operations available should be given to patients, with a discussion of the risks, potential complications and expected benefits. Patients should also be informed of the necessary postoperative diet and lifestyle changes. Patient discussions with a bariatric surgeon will provide more detailed information regarding operative issues.
A preoperative upper gastrointestinal endoscopy is performed, preferably by the surgeon, primarily to identify a hiatus hernia requiring repair at the time of bariatric surgery, to reduce the risk of postoperative gastro-oesophageal reflux disease. Endoscopy will also detect Barrett’s oesophagus, which is a relative contraindication to some operations. Preoperative assessment by the anaesthetist may require specific cardiac or respiratory tests.
Surgical options and current trends
In 2014-15, an estimated 22,700 weight loss surgical procedures were performed in Australia, an increase from 9300 in 2005-06 according to an Australian Institute of Health and Welfare report.19 More than 90% were performed in the private sector, highlighting the lack of government recognition for access in the public sector. Robotic bariatric surgery is reportedly equivalent but not superior to other types of minimally invasive bariatric surgery, although surgeons report benefits with regard to improved image quality and suturing.20
Biliopancreatic diversion with duodenal switch is not discussed in this article as the procedure is infrequently performed in Australia. However, there is increasing interest in this operation as it provides the greatest weight loss and improvement in comorbid conditions.21
Sleeve gastrectomy
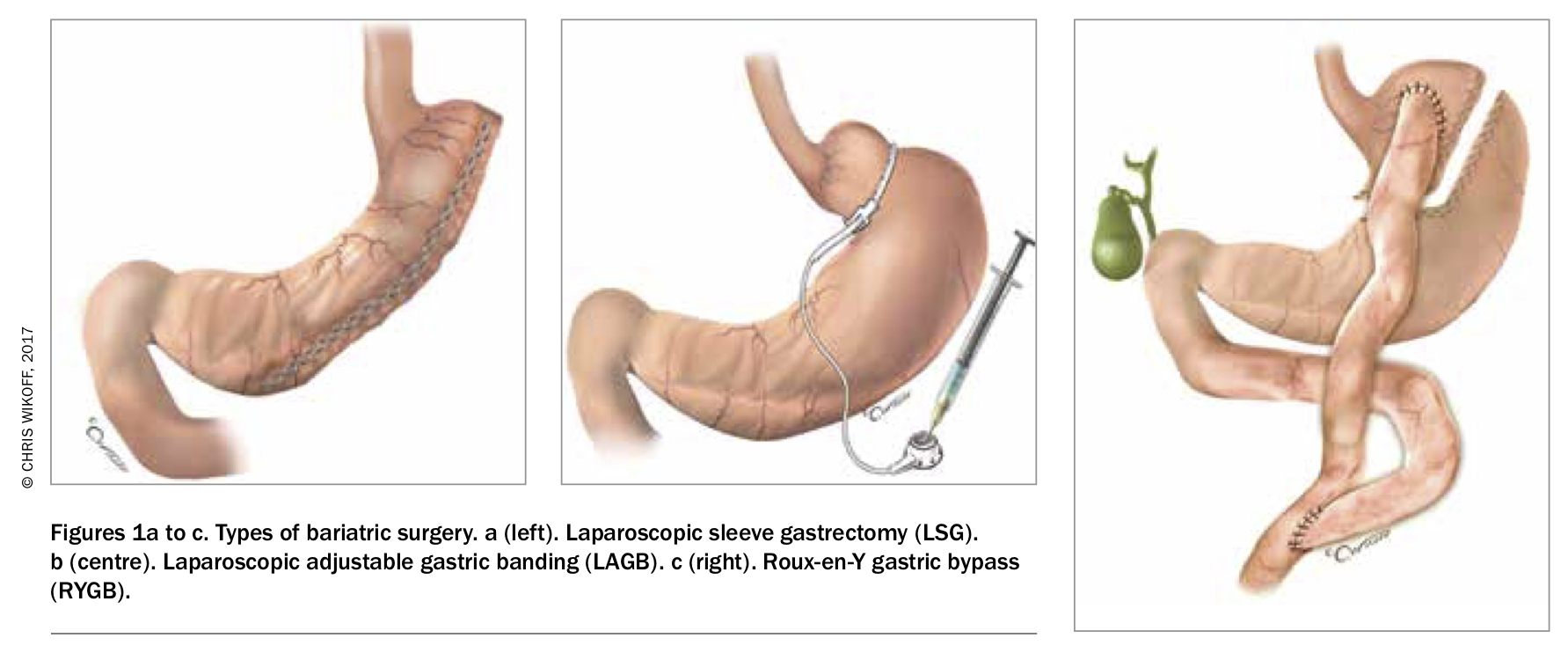
Sleeve gastrectomy is usually performed laparoscopically. In most patients, 70 to 80% of the stomach is removed by stapling parallel to the lesser curvature in a cephalad direction (Figure 1a). The pylorus is preserved, which reduces the risk and severity of dumping syndrome. As well as greatly reducing the gastric volume, sleeve gastrectomy only leads to several metabolic and hormonal changes. These include reduced levels of ghrelin (the hunger peptide), glucagon, glucagon-like peptide 1 and leptin.22 Initial weight loss is swift and sustained, with only minor weight gain after several years in most patients.23 The major complications of sleeve gastrectomy are staple line leak or bleed in the immediate postoperative period and gastro-oesophageal reflux as a later problem.
{kind=link}
Sleeve gastrectomy has become the dominant operation type in most industrialised countries including Australia.24 The reason is that it is more reliably effective than gastric band surgery, which was previously the most frequently performed operation but is now far less commonly performed. Sleeve gastrectomy has very similar effectiveness to Roux-en-Y gastric bypass (RYGB), with both operations providing more than 70% excess weight loss in a randomised trial.23 It is, however, significantly safer than the RYGB operation and avoids the long-term complications of the bypass operation.24,25
Laparoscopic adjustable gastric band
Following the first successful laparoscopic placement of an adjustable gastric band in 1995, uptake rates were high and promising initial results were reported (Figure 1b). Over time, the laparoscopic adjustable gastric band (LAGB) procedure has fallen out of favour because of problems with obstruction due to ingested food being stuck at the narrow lumen of the band, gastro-oesophageal reflux, which can be severe, and other complications including band slippage, band erosion and port and tubing problems. Although many patients have long-term satisfactory weight loss and control of obesity comorbid conditions, long-term failure of weight loss in up to 62% of patients has been reported.26
Patients with inadequate weight loss may have an overly tight band, which induces consumption of soft high-energy foods and drinks. In these patients, adjustment of the band fluid to an ideal volume combined with dietary advice may be sufficient to restart weight loss. In many other patients, however, band removal is performed, followed by a different bariatric operation.
Roux-en-Y gastric bypass
RYGB is more technically demanding and metabolically disruptive than sleeve gastrectomy, with significantly higher morbidity and mortality rates. This operation results in gastric restriction and intestinal malabsorption. The procedure involves restricting the size of the stomach by stapling to create a small proximal pouch; the bypassed stomach remains in situ and is subsequently difficult to examine endoscopically. A Roux alimentary limb of jejunum is anastomosed to the gastric pouch, with the biliopancreatic juice entering the bowel 50 cm or lower at a second anastomosis (Figure 1c). Malabsorption is therefore induced by bypassing normal absorption of ingested food in the foregut. Complications include anastomotic leak, internal herniation, bowel obstruction and nutritional problems due to the malabsorption.
Despite the higher morbidity and mortality profile of RYGB compared with either sleeve gastrectomy or LAGB, gastric bypass should be considered in some patients, such as those with markedly severe obesity, significant gastro-oesophageal reflux disease, especially with Barrett’s disease, and those with severe type 2 diabetes. A single anastomosis variant of the bypass operation is increasingly popular; high quality longer-term follow-up data comparing it with sleeve gastrectomy or RYGB are awaited, but it seems clear that there are fewer complications with the single anastomosis bypass operation compared with RYGB.
Follow up after surgery
In the early postoperative phase, patient progress is monitored closely with dietitian input. Patients progress from a fluid-only diet, to puree and soft food, and eventually to a relatively normal diet in most over the course of two to four weeks. Some patients report permanent inability to tolerate some foods such as steak or bread, especially in those who have undergone LAGB surgery. It is important that patients remain well hydrated and that protein intake is 60 to 80 g/day, for which commercially formulated liquid very low-calorie diet meals are useful.
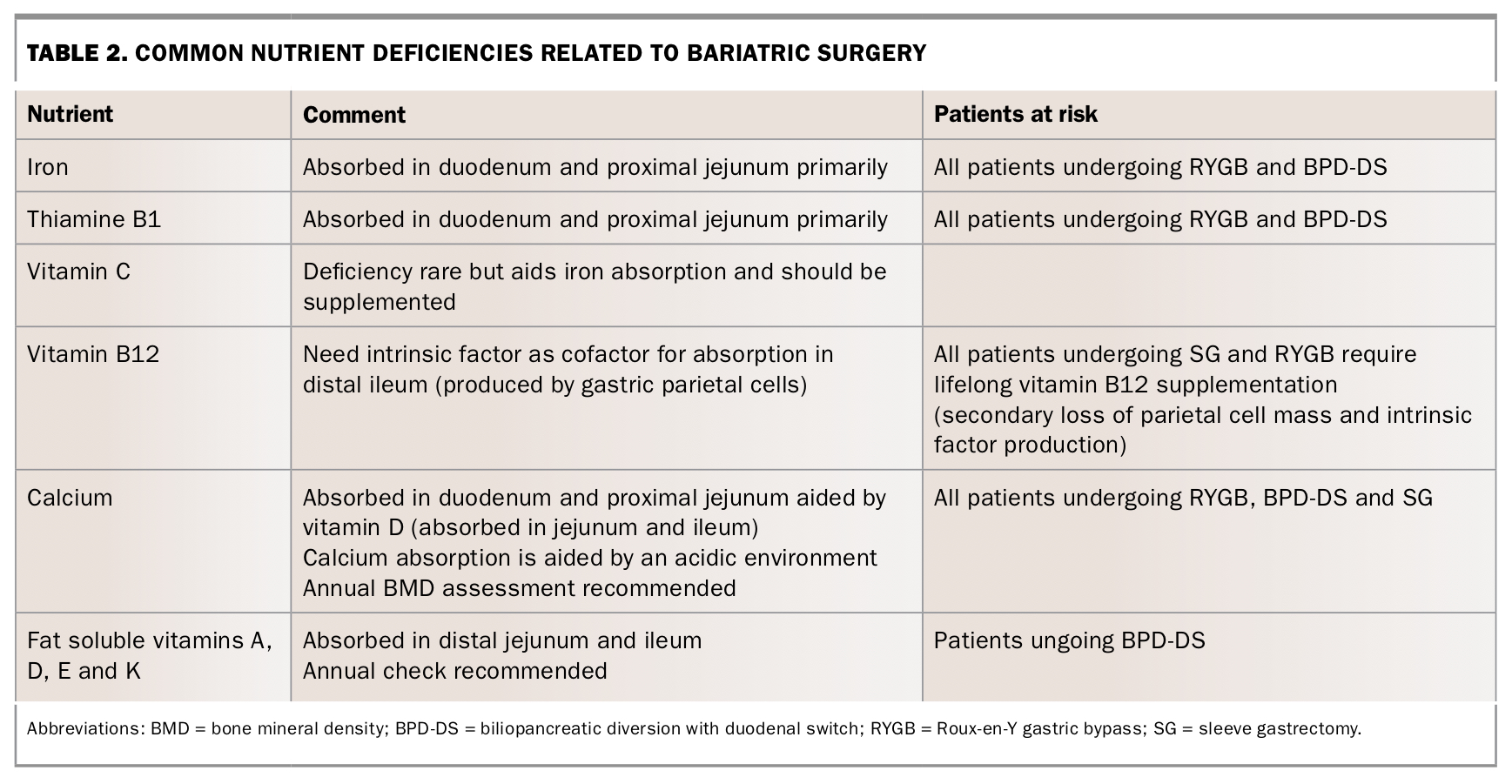
Deficiencies of many micro and macronutrients can occur postsurgery and monitoring for these should be undertaken. The most common deficiencies and patients most at risk are listed in Table 2. A typical set of blood tests for a patient who has undergone sleeve gastrectomy at six months, 12 months and annually thereafter includes a full blood count and measurement of albumin, calcium, magnesium, phosphate, folate, parathyroid hormone, 25-hydroxy vitamin D, iron, transferrin and vitamin B12 levels.
{kind=link}
Novel antiobesity procedures
It is important for GPs to be able to inform their patients that novel devices for obesity, outlined below, are neither restrictive (in the sense of decreasing oral intake) nor malabsorptive. Also, they go against the bariatric principles of healthy eating choices and modifications to diet that are the basis of durable medically meaningful weight loss management.
Intragastric balloons
Some patients who are unwilling to undergo surgery or do not meet the BMI and other criteria for surgery opt to have endoscopic placement of an intragastric balloon. The saline-filled silicone balloon within the stomach mimics gastric fullness. The treatment is temporary (six or 12 months) but may be repeated at intervals. Intragastric balloon treatment is not covered by Medicare or private health insurance and is consequently expensive. Initial weight loss should occur when used in concert with lifestyle changes, but weight regain is reported to occur in about one-third of patients after balloon removal, and weight cycling between serial procedures is common.27
Complications include pain, nausea and halitosis, as well as less frequently gastric erosion or ulceration, and perforation, which can be fatal. The balloon may also deflate and migrate, causing a bowel obstruction. The long-term efficacy of this procedure remains unclear, and safety notices have been issued by various government agencies worldwide regarding this therapy.
Endoscopic sleeve gastroplasty
Endoscopic sleeve gastroplasty (also known as transoral gastroplasty) uses endoscopic suturing to create a narrow gastric lumen that is intended to replicate a now discarded operation, vertical banded gastroplasty. The long-term failure of that operation suggests that patients who undergo endoscopic gastroplasty will need to be monitored for failure of the suture line. Intake is restricted and satiety following small meals occurs. Professional societies such as the American Society for Gastrointestinal Endoscopy suggest that endoscopists performing these procedures have a system in place for enrolment and long-term follow up of patients to monitor weight loss and maintenance.
Conclusion
In patients with obesity who have comorbidities such as type 2 diabetes, bariatric surgery has been demonstrated to be superior to intensive medical therapy in managing these diseases.16 Most patients will achieve at least partial remission of comorbid diseases, and normoglycaemia off all diabetes medications is also reported in most patients, but the diseases can recur if weight is regained. Bariatric surgical management has been shown to reduce all-cause mortality (including deaths due to diabetes, cardiovascular disease and cancer) in patients with obesity.28-33 It represents a growing area of experience for patient care, with good evidence to support certain bariatric techniques for sustained weight loss and improvements in overall health. An experienced team approach, tailoring treatment to the individual patient is important. If surgery is appropriate, the risks and benefits for each patient, including the psychological effects of permanent inability to eat a normal-sized meal, need to be considered and explained. At present, sleeve gastrectomy has the best risk-to-benefit profile. Patients must commit to lifelong adherence to dietary modifications and vitamin monitoring, as deficiencies are common.
Overall, obesity is a complex chronic disease for which specialist weight assessment and management clinics are required for optimal care. With the emergence of new drugs, devices and surgical procedures, as well as ever increasing patient numbers, assessment by teams skilled in this area is becoming more necessary. Surgery has a definitive effective role in management. Postsurgery diligent follow up and review of patient care is essential to maintain weight loss and remission of comorbid disease. MT