Adjunctive therapies for obesity: pharmacotherapy, VLEDs and bariatric surgery

Although lifestyle interventions remain the cornerstone of obesity treatment, this article highlights additional approaches to management that may help reduce and maintain weight. These adjunctive therapies include the role of the multidisciplinary team in obesity management, and the use of very low energy diets, pharmacotherapy and bariatric surgery.
- Obesity is a multifactorial disease requiring a comprehensive and often diverse management approach to both the disease itself and its related comorbidities.
- Adjunctive therapy, including pharmacotherapy and very low energy diets, can be used to aid weight loss and maintenance.
- Multidisciplinary obesity clinics are best placed to address the complex causes of obesity and its related comorbidities.
- Bariatric surgery should be considered for patients who have a body mass index 40 kg/m2 and over or 35 kg/m2 and over with comorbidities.
- Lifestyle intervention remains the cornerstone of treatment irrespective of the type of adjunctive therapy used.
Seeking effective solutions to obesity is arguably one of the greatest public health challenges currently facing Australia. Primary and community-based healthcare professionals are at the forefront of this challenge, often with limited time and resources to sufficiently address the multifactorial aspects of obesity management.
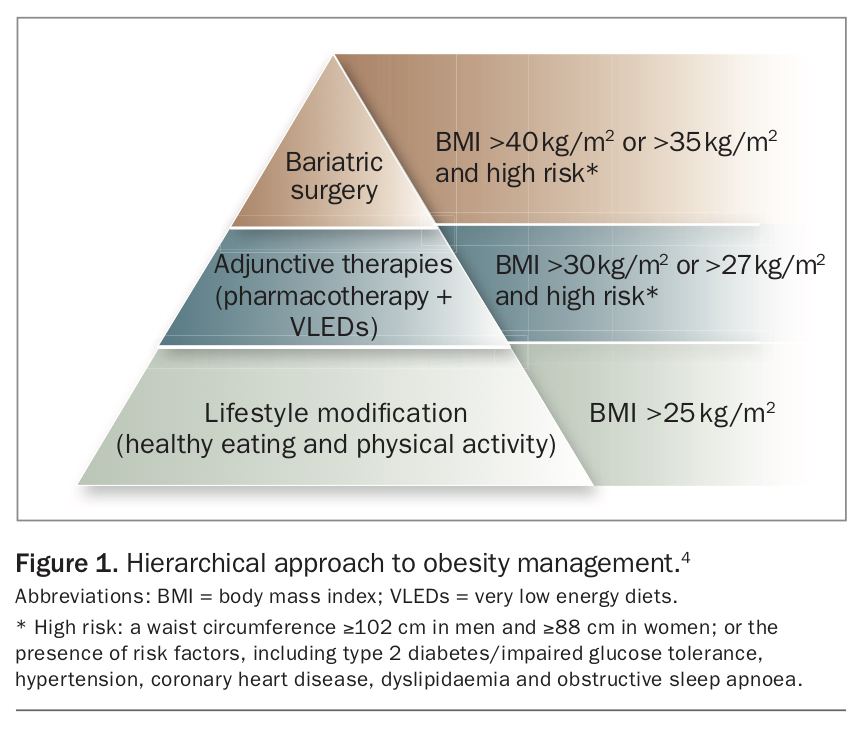
In the June 2020 issue of Medicine Today, we focused on practical approaches to lifestyle interventions for the management of obesity.1 The cause of obesity, particularly for patients with a very high body mass index (BMI), is multifactorial (e.g. periods of inactivity, disordered eating, medical problems, medications, genetics, lifestyle, physical and sexual abuse, etc.).2,3 It follows then that the management approach to obesity must address these many causes in addition to addressing obesity-related comorbidities. Although lifestyle interventions remain the cornerstone of obesity treatment, there are additional approaches to management, highlighted in this article, that may help reduce and maintain weight. These include the role of the multidisciplinary team in obesity management, in addition to the use of very low energy diets (VLEDs), pharmacotherapy and bariatric surgery. These adjunctive therapies should be considered when lifestyle interventions have failed to achieve sufficient weight loss or improvement in obesity-related comorbidities after a minimum of three months (Figure 1) or initially if the patient has obesity of grade II or above and psychological, financial and social barriers have been addressed.4 Ensuring the patient is ready to start adjunctive therapy is vital for success.
{kind=link}
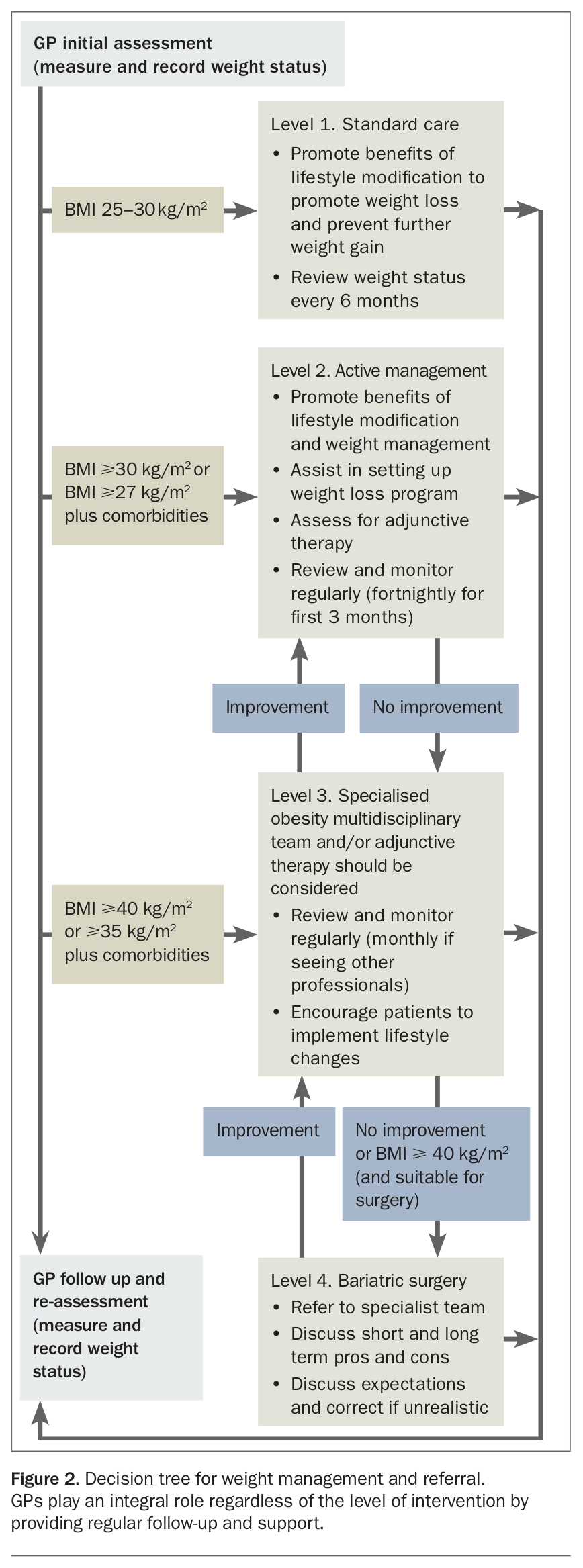
GPs play a crucial role in the management of obesity. They should aim to reinforce diet and exercise recommendations, and highlight possible lifestyle changes at each consultation in a nonjudgemental and empathetic way.5 Contrary to popular belief by GPs, most patients with obesity do want to discuss their weight with their doctor.6 GPs should also ensure there is adequate psychological support for the patient, and identify and manage obesity-related complications. The 2013 NHMRC clinical practice guidelines for the management of overweight and obesity can be used to inform and guide this process.7 These guidelines are structured according to the 5A’s (Ask, Assess, Advise, Assist, Arrange follow up), which has been shown to facilitate weight management by promoting physician–patient communication and emphasising follow-up care.5 Referral of the patient to a specialised obesity multidisciplinary team should be considered when the patient has multiple obesity-related issues or disease complications that require specialist expertise. Figure 2 outlines a recommended obesity referral pathway.
{kind=link}
Multidisciplinary specialist obesity clinics
Obesity is caused by a complex interplay of different aspects of a patient’s life, and thus the multidisciplinary team is well placed to deal with the multifactorial nature of obesity. The team uses diverse skills from multiple health disciplines, which usually include a medical practitioner, dietitian, physiotherapist or exercise physiologist, and psychologist. The aim is for the team to communicate regularly about the ongoing care of the patient and to identify and treat most, if not all, factors contributing to a patient’s excess weight. The team is also involved in screening, treating and/or facilitating specialist referrals for any obesity-related comorbidities. It is important that all members of the team communicate about all aspects of the patient’s obesity as issues will often cross disciplines. As we recommence care in the age of COVID-19 it is important to think of what changes may need to be made to the way we deliver obesity care. There will be less face-to-face interaction and more use of tele/virtual heath. Therapy groups will need to be run online via video conferencing facilities and there may need to be more, but shorter, contacts between such group meetings to help support people.
Interventions considered beyond lifestyle
Very low energy diets (VLEDs)
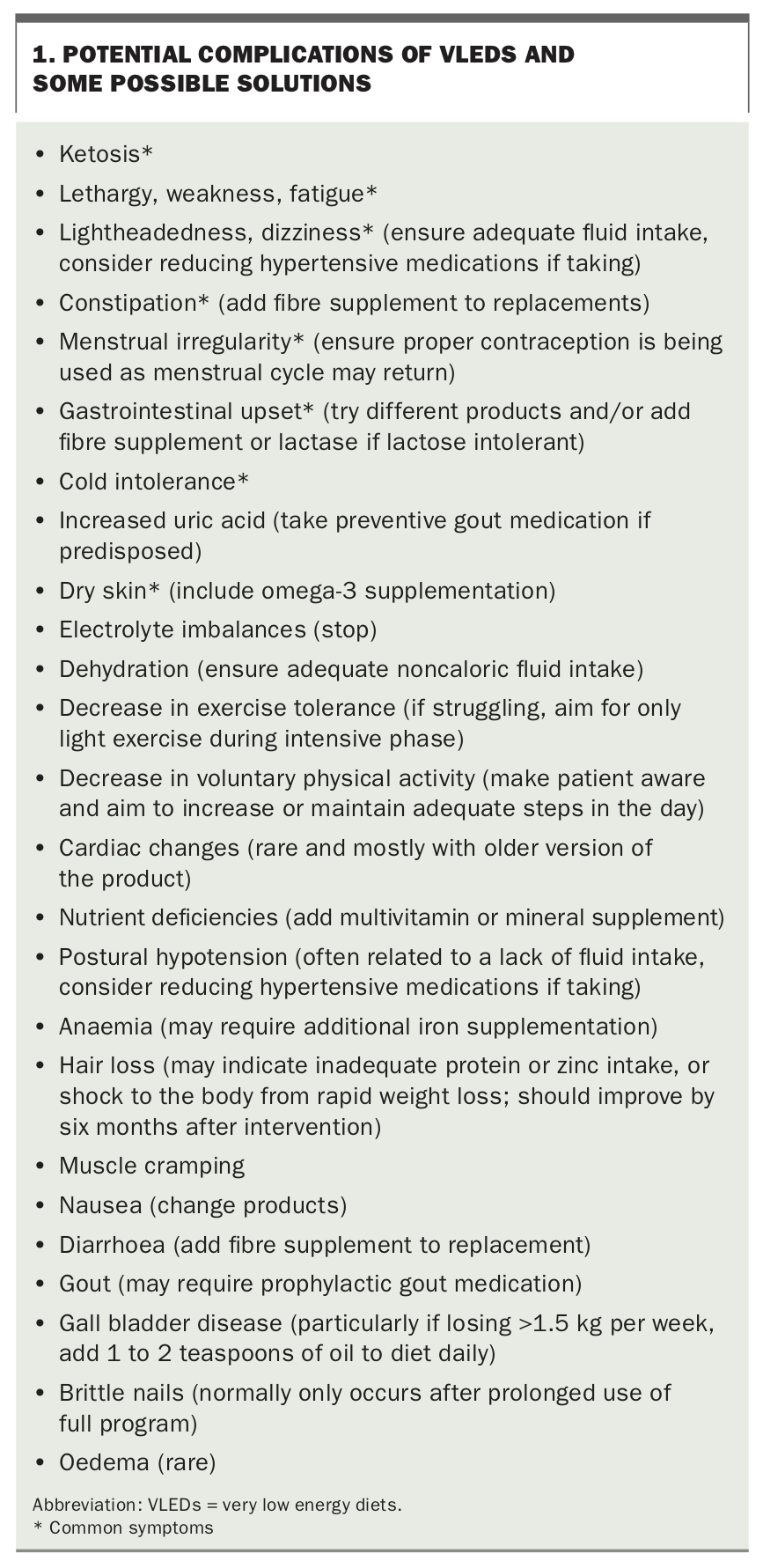
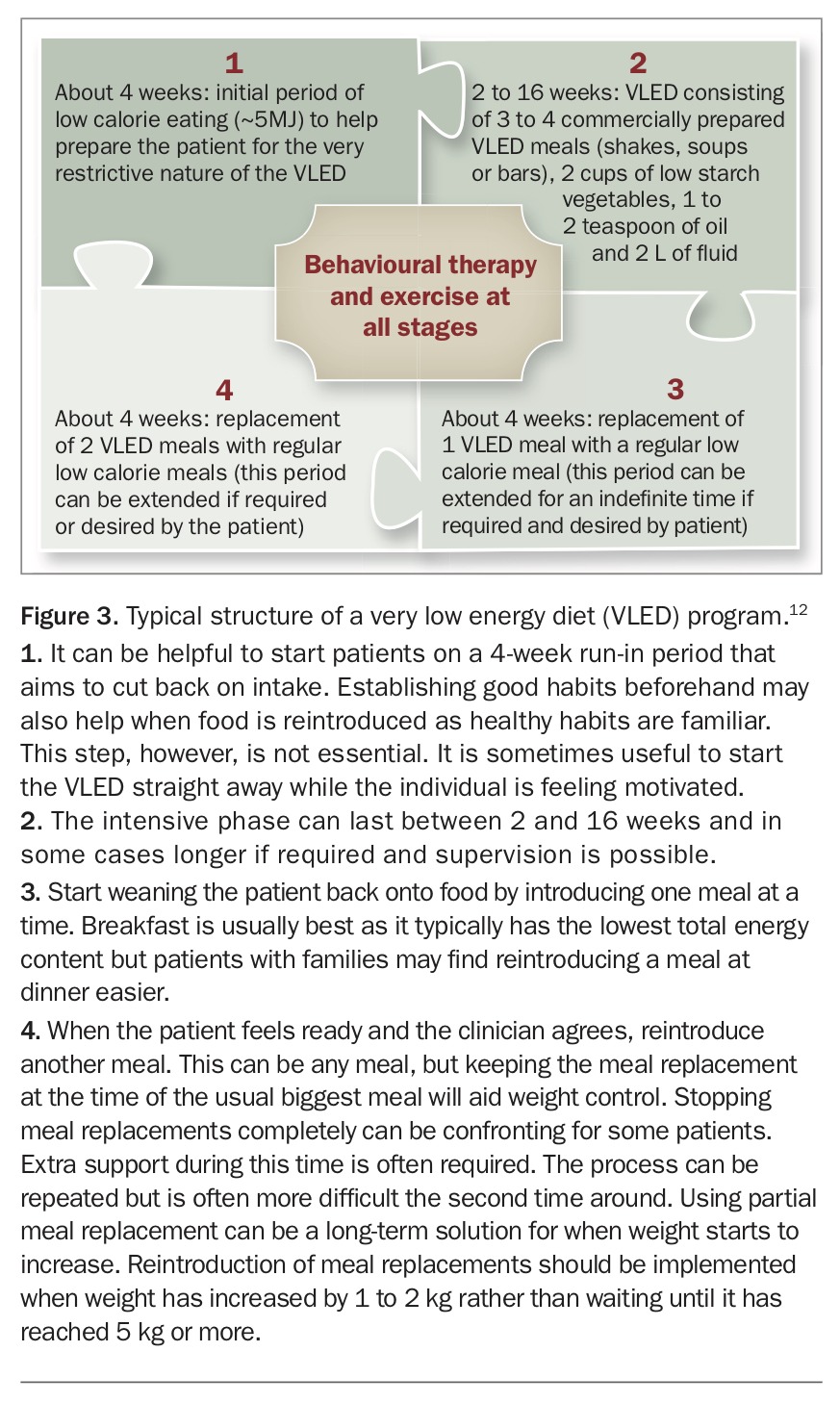
VLEDs, sometimes called very low calorie diets (VLCDs), are the most intensive dietary intervention for the management of obesity. This involves completely or partially replacing all usual food intake with nutritionally complete commercial products, which provide between 1845 and 3280 kJ (450 to 800 kcal) per day and are fortified with close to or above the recommended daily allowance of vitamins, minerals and electrolytes.8 The severe energy restriction results in rapid weight loss (which is very motivating for the patient), typically 1.5 to 2.0 kg for women and 2.0 to 2.5 kg for men per week.9 For instance, our recent review of VLEDs in people with class III obesity found a pooled average weight loss of 25.8 kg (95% confidence interval [CI],13.8 to 37.9 kg) in interventions lasting more than six weeks, representing about 10.2 to 28.0% weight loss.10 More weight is generally lost in the first one to two weeks due to increased fluid loss. However, the rate of weight loss subsequently slows due to a decrease in energy requirements, spontaneous physical activity and hormonal alterations and thus may not necessarily indicate a lack of treatment adherence.11 Although modern VLEDs are accepted as safe, there are several potential complications associated with them (see Box 1). VLEDs should ideally be started in consultation with a medical practitioner, particularly if the patient has comorbidities such as liver, renal, cardiovascular disease or diabetes. If initiated without medical supervision, support and encouragement from a health professional should not be underestimated, particularly during the weaning and weight maintenance phases. A typical VLED program is shown in Figure 3.12
{kind=link}
{kind=link}
Most commercial VLED preparations recommend three meals per day and provide about 70 g of protein. However, to attenuate the loss of lean body mass, aim for a minimum protein intake of 0.8 g/kg of body weight per day.13,14 Therefore, patients weighing over 85 kg may require four or more meal replacement sachets per day. Eating more than four meal replacements per day can be difficult due to their appetite suppressing effect and individual taste preferences. Alternatively, to keep total calories and carbohydrate intake low, a whey protein isolate supplement could be added to the VLED preparations or a small serving of lean protein could be included in addition to the meal replacements.13,14 Consideration of total energy intake should be kept in mind when prescribing additions to the basic program.
Patients often find the first three to five days of the VLED the most difficult as glycogen, then fat stores, are used for energy. This use of fat stores produces ketone bodies – leading to appetite suppression.15,16 However, even with ketosis it is difficult to completely replace all usual food intake and initiation of a VLED should involve discussion about filling in the time a patient would usually spend preparing and eating food, and what to do when socialising and eating with the family. One of the reasons VLEDs are effective is their restrictive nature, for they can take away the anxiety of deciding what to eat. Consequently, it is often when patients transition back to ‘real’ food that they will require the most support. VLEDs can be used intermittently (or partially) to help with weight maintenance.17
VLEDs have been used successfully in the primary care setting, with a mean bodyweight loss of 10.0 kg (standard deviation [SD], 8.0) at one year and 7.6 kg (SD, 6.5) at two years, and 24% and 11% of participants recording weight losses of 15 kg or more at one and two years, respectively.18,19 When compared with usual care for the treatment of diabetes, use of VLEDs have been shown to lead to greater diabetes remission rates at both one year (46% of participants in the intervention group vs 4% in the control group) and two years (36% of participants in the intervention group vs 3% in the control group).18,19
Weight reduction of 5 to 10% from baseline is associated with improvement in obesity-related comorbidities.20,21 Accordingly, as a VLED proceeds, ongoing review by a medical practitioner is recommended as antihypertensive therapy may need to be decreased and adequate fluid intake encouraged. In people with diabetes, their diabetic therapy almost always requires significant dose reduction and should be adjusted before starting a VLED with subsequent regular blood glucose level monitoring and ongoing dose titration in consultation with a medical practitioner. On average, a single serve of a VLED will contain between 17 and 24 g of carbohydrate, depending on the brand used.8 Although it only takes two weeks of use to see improvements in metabolic markers and reductions in liver fat, a recent meta-analysis has shown that, in those with class III obesity or above, it is optimal to stay on the product for a minimum of six weeks to achieve clinically significant weight loss of 10% or more.10,22 VLED programs can be run successfully by general practice nurses as shown in the DiRECT trial.18,19 Several publications provide more in-depth information on VLEDs.6,17,23
Pharmacotherapy
All interventions for the treatment of obesity are frequently limited by significant weight regain in the long term. For patients who already demonstrate good adherence to lifestyle modification or those who have lost a significant amount of weight but are struggling to maintain weight loss, pharmacotherapy can be an effective adjunct to their treatment. When pharmacotherapy is combined with lifestyle modification the proportion of body weight lost is usually 2 to 5% higher than with lifestyle modification alone (i.e. an initial weight loss of 10% vs 6%).24 In recent years, it has also been suggested that pharmacotherapy should be considered to prolong weight loss after bariatric surgery.25
Pharmacotherapy options remain limited in Australia. Phentermine monotherapy is approved but requires medical review every three months for ongoing use as an adjunct to lifestyle modification, usually starting at a dose of 15 mg daily and increased to 30 mg or 40 mg if required. Phentermine is associated with a 3.6 kg (95% CI, 0.6 to 6.0 kg) greater weight loss compared with placebo in major studies and, before the recently US Food and Drug Administration-approved combination therapy phentermine/topiramate ER (not available in Australia), phentermine monotherapy was the most effective obesity pharmacotherapy for both weight reduction and improvement in comorbidities.26,27 Phentermine causes appetite suppression; however, its use is often associated with poorly tolerated adverse effects relating to its stimulant properties, including dry mouth, agitation, insomnia and decreased concentration. Of greatest concern is its effect on cardiovascular risk factors – in particular, blood pressure and heart rate. For this reason it is contraindicated in individuals with hypertension, existing heart valve abnormalities or heart murmurs, cerebrovascular disease or severe cardiac disease (including arrhythmias and advanced atherosclerosis). Long-term clinical trials also indicate increased tolerance and habituation associated with prolonged use, and phentermine is not recommended in people with psychiatric disorders, including anorexia or depression, or in those at risk of drug dependency.28,29
Orlistat is a gastrointestinal lipase inhibitor that reduces the amount of fat absorbed from the diet by about 30%, leading to weight loss through reduction in total energy intake. Orlistat is associated with 2.89 kg (95% CI, 2.27 to 3.51 kg) or 2.9% (95% CI, 2.3 to 3.4%) greater reduction in body weight, in combination with lifestyle modification, compared with placebo.30,31 Initially available only with a prescription, it was reclassified as a ‘pharmacist-only medicine’ in 2003. It is currently available over the counter in 120 mg capsules (84 capsules per pack) and patients are advised to take one with every meal. It remains the only obesity therapy with long-term safety and efficacy data. However, its clinical use is predominantly limited by its gastrointestinal side effects, including increased defecation, liquid/oily stools, anal leakage, increased urgency and flatulence. Although these symptoms are significantly reduced on a low-fat diet, patients often will avoid taking the tablet with high-fat foods rather than changing their diet. If patients have not lost weight within the first three months of starting orlistat it is unlikely that it will have a significant benefit.
Liraglutide is a glucagon-like peptide-1 (GLP-1) receptor agonist that was previously approved for the treatment of type 2 diabetes, at a dose of 1.8 mg daily. It has now been approved at a higher daily dose (3 mg) for the long-term treatment of obesity. Liraglutide is injected once daily subcutaneously into the abdomen, thigh or upper arm. Weight loss with liraglutide appears to be due to both central and peripheral effects leading to delayed gastric emptying, reduced appetite and energy intake.32,33 Studies directly comparing liraglutide with orlistat in conjunction with lifestyle intervention in adults with overweight or obesity but without diabetes showed that the mean weight loss with liraglutide (3 mg dose) was 7.2 kg, compared with 4.1 kg for orlistat and 2.8 kg for lifestyle intervention alone.34 This weight loss was essentially maintained over a two-year period.35 Liraglutide is commonly associated with gastrointestinal adverse effects that are generally self-limiting, hypoglycaemia and headache. Liraglutide is also associated with central nervous system effects, including fatigue, dizziness, insomnia, suicidal ideation and depression. Allergic and injection site reactions can also occur.
Naltrexone hydrochloride and bupropion hydrochloride extended release 8/90 mg combination therapy is the most recent obesity pharmacotherapy approved in Australia. It is thought to act centrally to reduce hunger and control cravings and eating behaviour.36 Weight loss of 9 kg versus 5.2 kg for lifestyle intervention alone has been reported for this therapy, with placebo-corrected weight reduction from baseline of –3.2%.37 Common side effects include constipation, headache, nausea, dizziness, insomnia, dry mouth and diarrhoea. Contraindications are seizure disorders, uncontrolled hypertension, acute alcohol or benzodiazepine withdrawal or dependence, bipolar disorder, concurrent treatment with bupropion or naltrexone, current dependence on chronic opioids or opiate agonists, eating disorder, pregnancy, severe hepatic impairment, end-stage renal failure and concurrent therapy with monoamine oxidase inhibitors. The dose should be escalated over a four-week period from initiation, starting at one tablet in the morning for one week, and the maintenance dose from week 4 onwards is two tablets in the morning and two at night.
Surgery
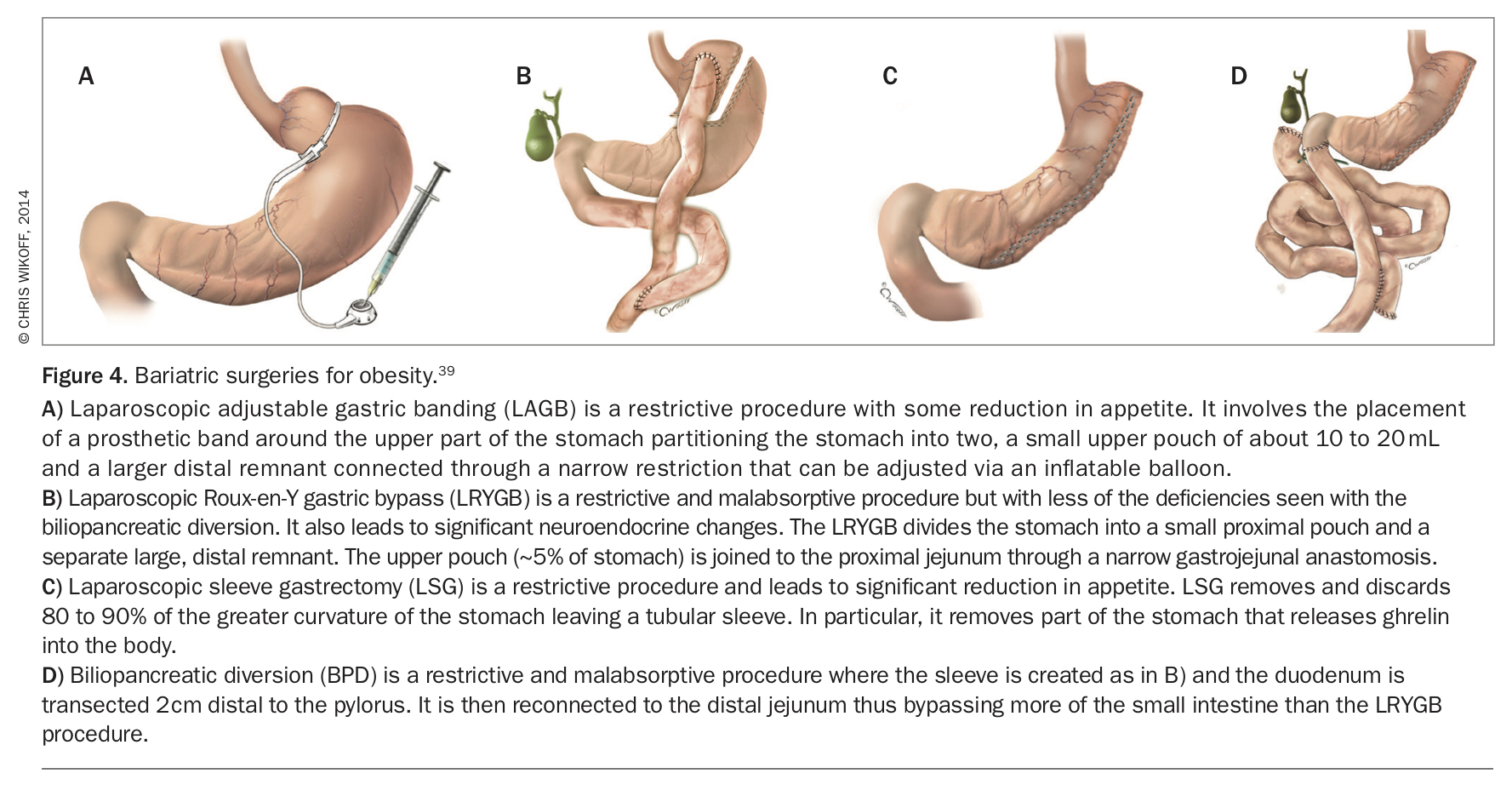
The most common surgeries offered in Australia for obesity are laparoscopic sleeve gastrostomy (LSG), laparoscopic adjustable gastric banding (LAGB), laparoscopic Roux-en-Y gastric bypass (LRYGB) and the newer omega loop or mini bypass (OLGB), which is similar to RYGB but involves one anastomosis rather than two and has a shorter surgery time (Figure 4).38-40 The bilio-pancreatic diversion (BPD) with or without duodenal switch (DS) was a common bariatric procedure worldwide; however, it is now less commonly performed due to the increased risk of complications and nutritional deficiency long term. These surgeries were previously thought to be purely restrictive or malabsorptive procedures; however, it is now recognised that they have significant neuroendocrine implications that affect intake and metabolism.41
{kind=link}
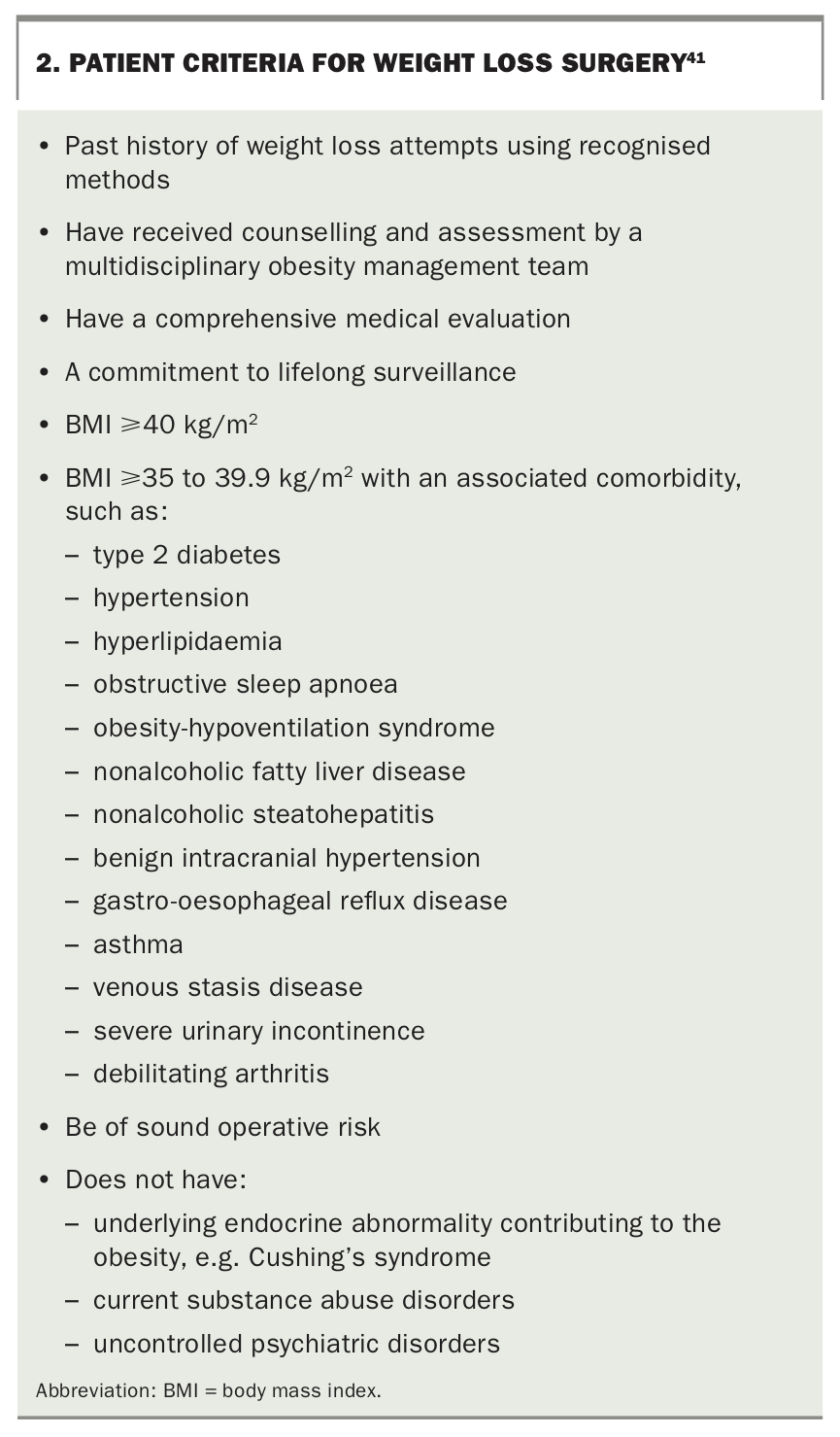
Bariatric surgery helps people to feel satisfied with a smaller amount of food. The suggested criteria to determine suitability for surgery is outlined in Box 2.41 Surgery has been shown to lead to greater weight loss and improvements in comorbidities than lifestyle change alone. Most of the weight loss occurs in the first 12 months; subsequently, weight will generally plateau or start to increase regardless of the type of surgery used.42 Some patients do eventually regain all lost weight. However, the average weight loss achieved is 15 to 40% of baseline weight or 12 to 17 BMI units depending on surgery type.42-45 Malabsorptive procedures (BPD DS, LRYGB and OAGB) are generally regarded as producing greater weight loss and improvement of obesity-related comorbidities.6,40,44-47 However, the average amount of weight loss produced by all surgeries varies significantly between studies and may depend on the team involved.6,46,48,49 One study showed that 10% of patients had lost about 12% or less of their starting body weight 12 months after sleeve gastrectomy.50 Despite patient expectations, most individuals remain in the obese if not severely obese category after surgery. In addition, weight regain is common and some patients end up as heavy as they were before surgery.
{kind=link}
Poorer prognosis with regards to maintenance of postsurgical weight loss has been associated with older age, binge eating, emotional eating, grazing, sweet cravings, a lack of control around eating, a lack of exercise, a lack of support, increased ghrelin levels and the severity of the surgery (e.g. size of the sleeve or amount of gastrointestinal track bypassed).51-54 Lifestyle modification therefore remains crucial, even after surgery. In addition, diet quality and lifelong micronutrient supplementation becomes important due to the reduced intake. Micronutrients should be checked before surgery and corrected to decrease risk of nutrient deficiency after surgery. In particular, levels of vitamin D, iron, B12, folate and calcium should be checked because they are often low in obese individuals and/or can be affected particularly by the more malabsorption surgeries. Presurgery deficiencies may increase the risk of postsurgical anaemia and osteoporosis.55-58
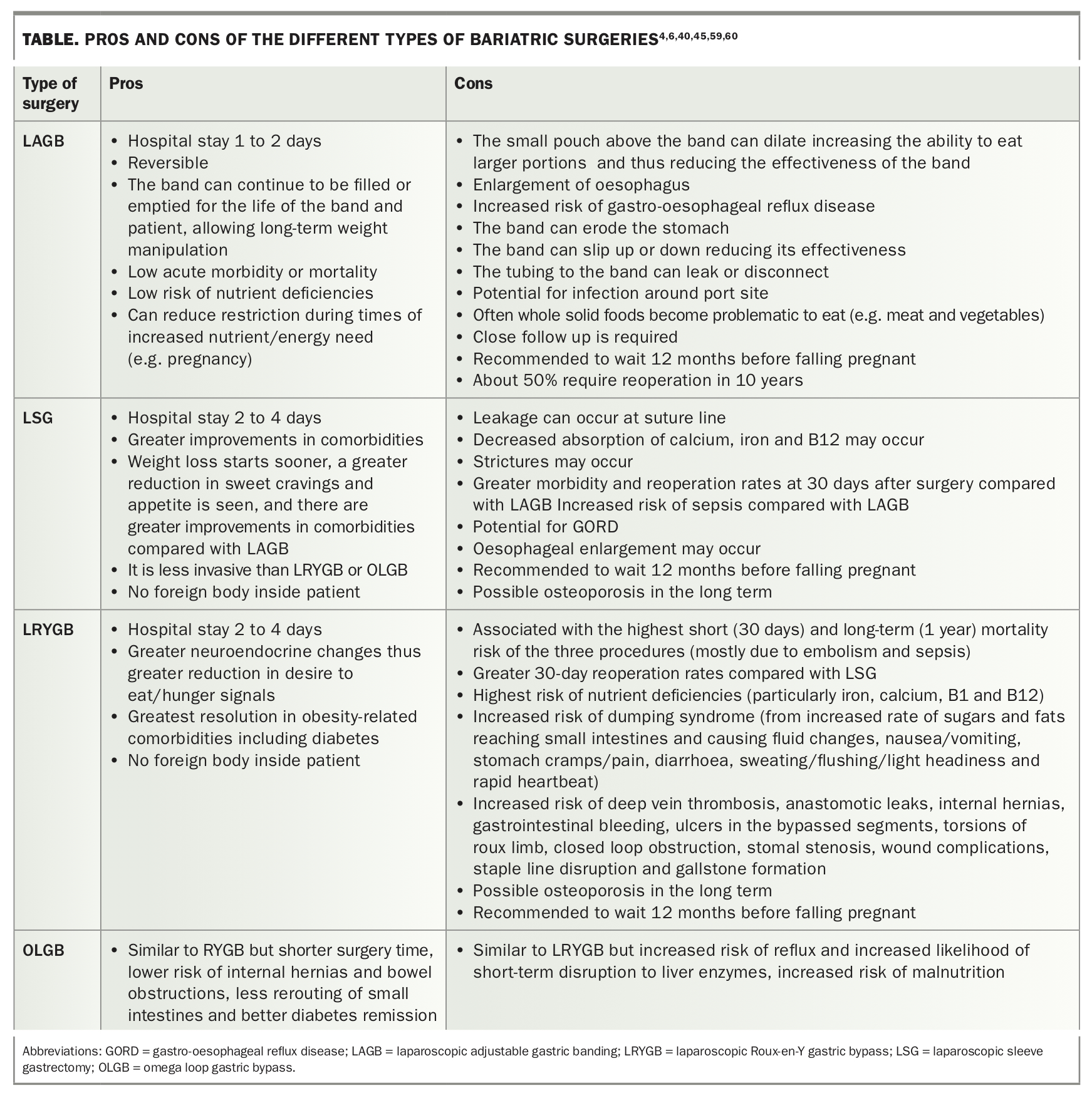
Many patients have unrealistic expectations relating to outcomes from surgery. For example, although it is generally emphasised in education before surgery, patients often think they can return to old habits and ignore the long-term commitment to lifestyle change. Poor food choices can lead to weight gain over time even if portions are small. Patients may also not fully appreciate the ongoing medical management that is required. The pros and cons of surgery should be repeatedly discussed with patients, as should the wider social, dietary and psychological implications (see Table).4,6,40-46,55-60 This is often best done with a multidisciplinary team but should also be covered by all health professionals involved with the patient’s care, especially the primary physician.
{kind=link}
Conclusion
Obesity is a multifactorial disease requiring a comprehensive multidisciplinary management approach to both the disease itself and its associated comorbidities. VLEDs, pharmacotherapy and bariatric surgery represent effective adjuncts to ongoing lifestyle modification and may be used as either single therapies or in combination throughout the patient’s life, reflecting the nature of obesity as a chronic illness. Nevertheless, lifestyle modification remains the cornerstone of obesity therapy, particularly in maintenance of weight loss. A multidisciplinary team within a tertiary obesity service is frequently best placed to address the complex causes of obesity and its related comorbidities for an individual patient. However, this approach will be most effective in the long term when supported by the GP in the primary care setting. MT
References
DrugsAdvisoryCommittee/UCM218824.pdf (accessed February 2014).
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.