‘On call’ – telehealth consultations during COVID-19

This series highlights common medicolegal issues in general practice. Written by a team from medical defence organisation Avant, the series is based on actual situations, with details changed for privacy and some issues summarised for the sake of discussion. This scenario explores the emerging issues for GPs, who are rapidly having to adapt to telehealth consultations during the COVID-19 pandemic.
Although telehealth was well established in some communities before the COVID-19 pandemic, the move to almost exclusively technology-based consultations over the period of a few weeks has been a sudden shift for many medical practitioners and patients. Processes had to be implemented quickly and with a sense of urgency. Some weeks after the initial emergency, doctors and practices are gradually working through the processes and support they need to provide patient care effectively without face-to-face consultations. As GPs providing telehealth consultations and responding to concerns and queries to our medical defence organisation, we discuss our insights and suggestions for addressing some of the issues we have encountered.
Case scenario
Late in the afternoon, Dr Ell is running about 25 minutes behind with her appointments. She telephones the last patient of the day who has requested a telehealth consultation. The patient, Peter, announces that his gout has flared up and he needs a repeat of his usual medication.
Dr Ell identifies Peter as a regular patient of the practice, starts to explain the limitations of the telehealth consultation and asks about the availability of a video consultation. Peter says he understands, but the consultation will need to be by telephone. He is looking after his grandchildren, and they are in the car on the way to their mother’s home.
He says, ‘It’s exactly the same as the last five times. That joint in my right big toe is swollen and red and hot. I’m supposed to go back on shift tomorrow but I can’t go in because I can’t get a boot on, so I just need another script for the usual stuff and a medical certificate.’
According to his medical records, Peter is in his late 50s and works in the construction industry. He has a history of long-standing type 2 diabetes mellitus treated with insulin, hypertension and gout. He has had several episodes of gout over the past few years, slowly increasing in frequency. He has been prescribed naproxen on multiple occasions.
Peter admits to having binged over the weekend on cheap lobster and beer. He says that when he woke up this morning, his foot felt as if he had dropped a load of bricks on it, but he is sure it has not been injured. Dr Ell asks if he has had any fever or other symptoms, and he says he feels fine.
Dr Ell decides to treat Peter for acute gout and confirms the details of his pharmacy so she can send a prescription for naproxen. She checks Peter’s email address from the file and confirms he is happy to receive the medical certificate by email. She is reminding him to call back if the pain does not start to resolve, when Peter breaks in. ‘Yes yes, thanks doc. I’ll have it with food. Got to go. The kids are about to murder each other. I’ll be fine now, thanks.’
Medicolegal issues
Is a telehealth consultation appropriate?
Broadly speaking, telehealth could involve using any form of telecommunications technology to conduct a consultation with patients, including videoconferencing or telephone.
During the COVID-19 pandemic, the Australian Government Department of Health has created temporary MBS item numbers that can be used to bill for telehealth consultations. These item numbers require consultations to be provided using either the telephone or videoconferencing software. The Department has stated that videoconferencing is the preferred approach. However, during the COVID-19 pandemic, practitioners may offer telephone services if videoconferencing is not available.
The Medical Board of Australia guidelines for technology-based consultations outline the steps and standards of care medical practitioners are expected to follow.1 The guidelines emphasise that a consultation may be conducted by telehealth only if the doctor is satisfied it is safe and clinically appropriate to do so. This assessment can be a challenge for practitioners who need to weigh up the risks and benefits of a face-to-face consultation against the constraints of the technology. When patients are unable or unwilling to connect via videoconference, then doctors do not even have the opportunity to view the patient or their presenting issue.
Is a physical examination needed?
Practitioners using telehealth have identified strategies to assess the patient’s condition and symptoms.2 For example, the patient’s demeanour and skin features may be visible during videoconferencing, and the patient can be asked specific questions about physical signs and to take readings with any instruments they have at home, such as temperature, pulse and blood pressure.2 However, the Department of Health has confirmed doctors using telehealth item numbers must also be able to make arrangements for patients to have a face-to-face consultation if the patients require a physical examination that cannot reliably be conducted remotely.3
It is not essential that the practitioner who conducted the telehealth consultation also provide the face-to-face consultation. Practitioners who are vulnerable or in a different physical location to the patient may need to arrange a referral to a colleague or involve another health practitioner, such as a community nurse or allied health practitioner. However, it is important that practitioners can comply with the professional requirement to make appropriate arrangements to follow the progress of the patient, inform the patient’s GP or other carers and keep colleagues well informed when sharing care.2
The Department of Health has made it clear that telehealth consultations can be billed only when the health practitioner has the capacity to provide the full service safely and the service is clinically appropriate. Be aware that if you are unable to complete a consultation via telehealth without a physical examination and arrange for a colleague to see the patient, your colleague’s consultation may be considered a continuation of the same consultation, in which case it cannot be billed as a separate item number.4
What consents are required for telehealth?
Patients need to give their informed consent to the consultation being conducted by telehealth rather than face to face. The consent process should involve discussing with patients the risks and benefits of telehealth, including its limitations. A patient’s verbal consent at the time of the consultation is sufficient and should be recorded in the patient’s medical record.
Practitioners also need the patient’s informed financial consent before providing the service. Specifically, you need to explain whether the telehealth consultation will be bulk-billed or whether some or all of the fees will be billed as an out-of-pocket expense.
How can patient privacy be ensured?
A challenge that practitioners have noted with telehealth consultations is maintaining patient privacy. Practitioners consulting away from their practice need to take particular care to ensure that no-one else can see their monitor or overhear their call and to make sure that records (whether physical or electronic) are secure.
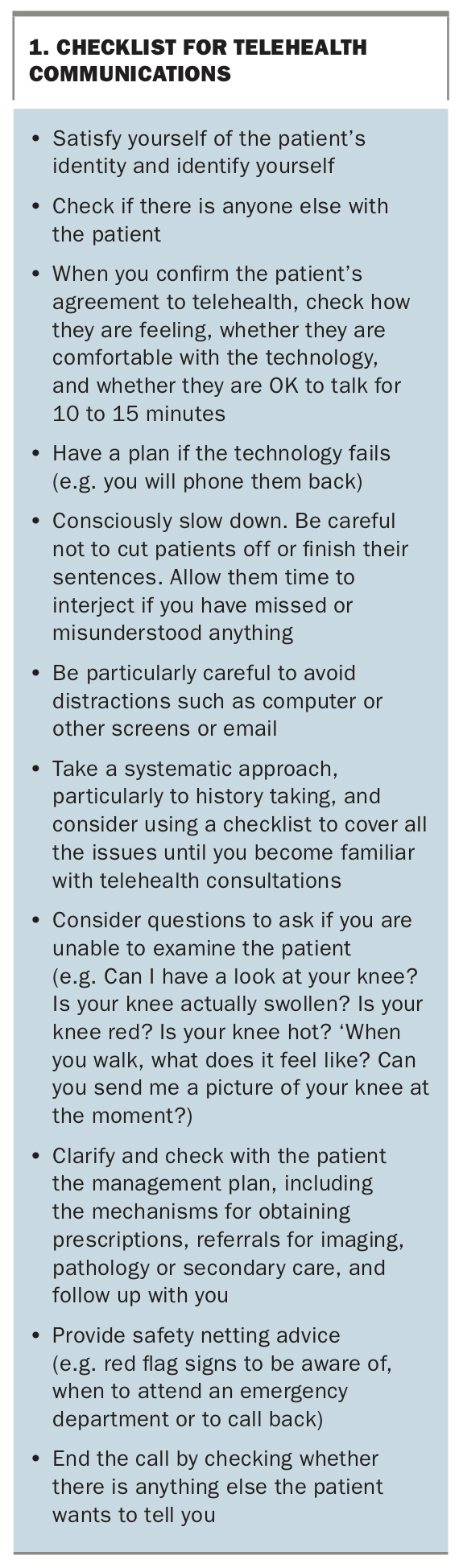
However, practitioners may also need to check that patients realise they may need privacy for the consultation and that it may not be appropriate to discuss health issues in a public place or where others can overhear. This may be a particular concern for young patients, or those at risk of violence or abuse.5 Some questions that might flag that privacy is a concern are included in the checklist for telehealth communication in Box 1.
{kind=link}
How can prescriptions, tests and referrals be managed?
When determining whether to prescribe after a telehealth consultation, practitioners need enough information to satisfy themselves that the prescription is appropriate and not contraindicated.6 Having sufficient information about the patient’s presenting complaint, medical history and current medical conditions and medications is crucial. This is particularly important if the patient is new to the practice or practitioner.
In addition to the clinical issues, practitioners need to consider the practical question of how the patient will access any medication. The Department of Health expects electronic prescribing technology will begin rolling out in mid-2020.
As an interim measure, changes to the PBS and amendments in most states and territories allow pharmacists to dispense medications (except S8 and S4D medications) based on a digital image of the prescription (‘image-based prescribing’). Under these arrangements, the prescribing doctor must still sign a hard copy prescription. The practitioner can create a digital image of the prescription (by scanning or photographing the hard copy) and send it to the patient’s pharmacist via email or fax. Practitioners must keep the paper prescription for at least two years from the date of the prescription for audit purposes.7 However, the rules are currently complex and changing; some states allow image-based prescribing of S8 and S4D medications, whereas others do not. It is important to check the current rules in your state or territory.
Alternatively, some practices have a system where the patient collects the prescription from the front desk, provided it is safe to manage prescriptions in this way.
Practitioners can order tests such as pathology or diagnostic tests or arrange specialist referrals via email or mail and in consultation with the patient. During a telehealth consultation, practitioners should take the time to explain to the patient the importance of any tests or referrals, as well as clarifying any referral arrangements in the same way they would in a face-to-face consultation.
Discussion
As the new telehealth services have rolled out during the COVID-19 pandemic, it appears that most patients and practices have been finding telephone consultations more accessible than videoconferencing. Practitioners have reported feeling more drained than usual by the effort of interpreting a patient’s symptoms over the phone without any visual or nonverbal cues. Practices and patients are increasingly shifting to videoconferencing, which allows a more complete patient assessment but still requires increased care so as not to miss nonverbal cues.
Practitioners are also reporting a significant number of consultations with patients experiencing mental health issues and the need to spend considerable hours managing the additional administration requirements of telehealth consultations. This includes verifying patient identity, confirming consents, double-checking email and contact details, checking with pharmacies and scanning and emailing prescriptions. It may be almost a relief when a known patient presents with an apparently simple issue.
It is nevertheless important, even more so when the patient cannot be examined, to consider differential diagnoses and ensure you look for any red flags to avoid missing significant diagnoses. Clear articulation of ‘safety netting’ is even more important than usual.
Follow up
Appropriate follow up and effective safety netting are crucial to ensuring patient safety. GPs need to make sure that patients are clear about how and when they should follow up and what has been agreed about monitoring test results or recalling the patient. Make sure they are clear about how they should monitor their condition and what to do if it deteriorates.
This might be particularly challenging when patients appear distracted and may not be giving you their full attention. Consider whether it would be helpful to send a follow-up email or message to the patient reinforcing your advice. If so, ensure you use a generic practice email address that makes it clear the address is not monitored to avoid ending up in a ‘consultation via email’ situation. Consider even rescheduling the appointment to a more convenient time when the patient can focus fully as they would during a face-to-face consultation.
Maintaining medical records
Clear and careful documentation of consultations will be extremely important. Making sure you and all practitioners involved in the patient’s care can access up-to-date medical records is essential to ensuring patient safety and continuity of care. If you are working away from the practice, you will need to have a plan for accessing and updating patient records.
If there are ever any questions about the consultation, why you reached a particular diagnosis and treatment plan, or what you discussed with the patient, having a clear record will be particularly important. The Medical Board of Australia has stated there will be no ‘watering down’ of professional standards during the COVID-19 pandemic.4 However, the Board has also said that ‘If a concern is raised about your decisions and actions, as always, the specific facts will be considered, including the factors relevant to your working environment. We would also take account of any relevant information about resources, guidelines or protocols in place at the time.’8
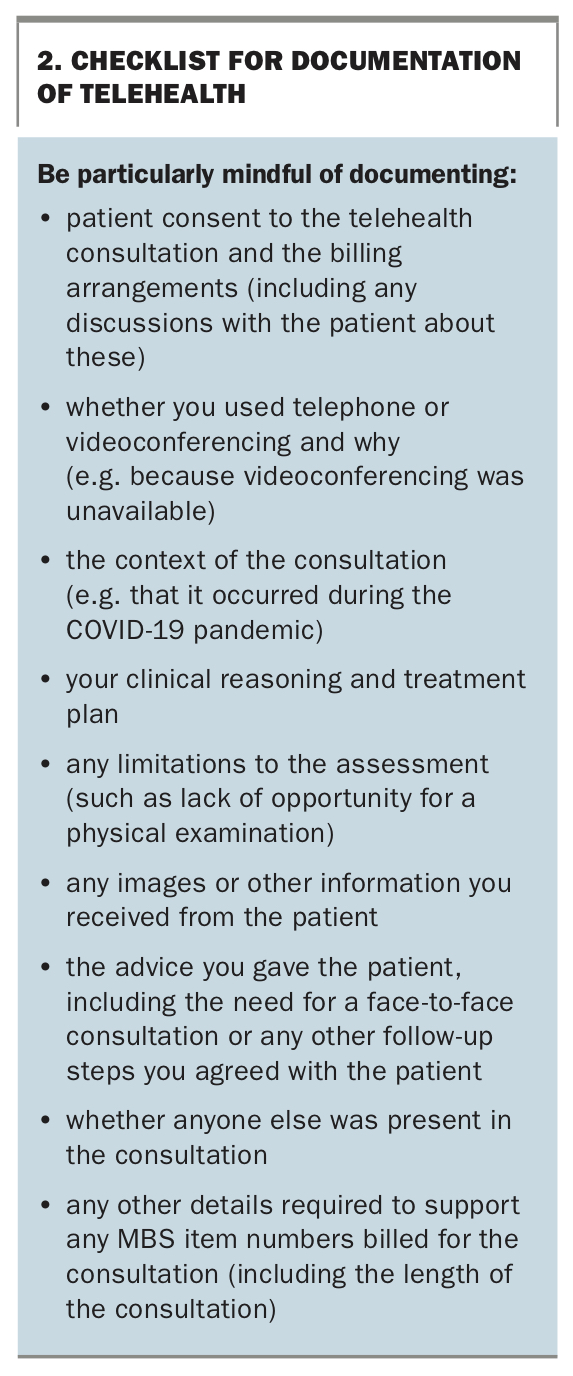
A checklist for documentation of telehealth consultations is outlined in Box 2.
{kind=link}
Communication – more important than ever
Much of a consultation involves absorbing information through visual cues, often subconsciously: how a patient walks into the consultation room, how they sit down, how they present and their demeanour during the consultation. Trying to find a substitute for this in a videoconference or telephone call may feel like learning to practise all over again. It may be easy to miss things that might be second nature to check or consider if the patient were in front of you.
Slowing down and thinking consciously about your communication can be hard when a patient is sounding rushed and distracted, but it may also be the key to a satisfying and effective consultation. Consider strategies such as a systematic approach, particularly to history taking, or even using a checklist and systems review to cover all the issues until you become familiar with telehealth consultations. Additional strategies to help address the communication challenges, particularly for telephone consultations that lack visual cues, are included in Box 1.
Recording the consultation
Whether patients or doctors can record consultations is an issue that arose frequently, even before the current expansion of telehealth.9 Recording a consultation without permission may be an offence, but the law on this is complex and each state’s legislation is slightly different. Practitioners should seek advice or contact their medical defence organisation if they have any concerns. However, if you and the patient agree that it would be helpful to record the consultation, make sure you discuss and get clear, documented agreement on how the recording can be used. Always keep your copy of the recording in the patient’s medical record.
Outcome
After Dr Ell completes the phone call with Peter, she cannot shake the feeling she missed something. Did she specifically ask about fever or chills to rule out anything more sinister? She notices Peter has not had a diabetes review in some time. She makes a note to check on him again. When she manages to catch Peter alone two days later, Peter says he actually has been feeling a bit feverish but did not want to say anything in front of his grandchildren who were anxious about him getting COVID-19. He assumed it was another symptom of gout and did not realise it could be anything more serious. He mentions that he has noticed a bit of discharge in his sock and is not sure whether this is related to the gout.
Dr Ell is concerned that there might be more to the presentation than gout and arranges for Peter to attend the practice to be reviewed by a colleague. Her colleague Dr Jay notes that Peter looks a little pale. Examination shows he has a fever (temperature, 38.2 degrees) and mild tachycardia (heart rate, 110 beats per minute). A finger prick blood sugar measurement shows a blood glucose level of 14 mmol/L. Dr Jay notes a small sloughy ulcer on the base of Peter’s right great toe, surrounded by an area of redness that has started to spread towards his ankle. Dr Jay suspects an infected ulcer with surrounding cellulitis and arranges hospital admission for Peter.
Conclusion
Telehealth has benefits because it enables medical practitioners to provide health care to patients in an environment where both practitioners and patients can be vulnerable. However, it needs to be undertaken safely. Effective care via telehealth depends on the quality of the data the practitioner is able to collect from patients without being able to see them in person. GPs must be confident that they have the capacity to provide the full service safely and that the service is clinically appropriate.
If as a GP you have concerns about the quality of the information you have been able to obtain or are not satisfied that you have sufficient information to formulate a diagnosis or a plan for investigating potential diagnoses then the consultation may not be one that can safely be conducted via telehealth. An initial treatment with effective safety netting and a clear plan for follow up may reassure you that your care was appropriate. However, if you have any concerns that the patient may need a physical examination that cannot reliably be conducted remotely, you need to be able to arrange for patients to have a face-to-face consultation.
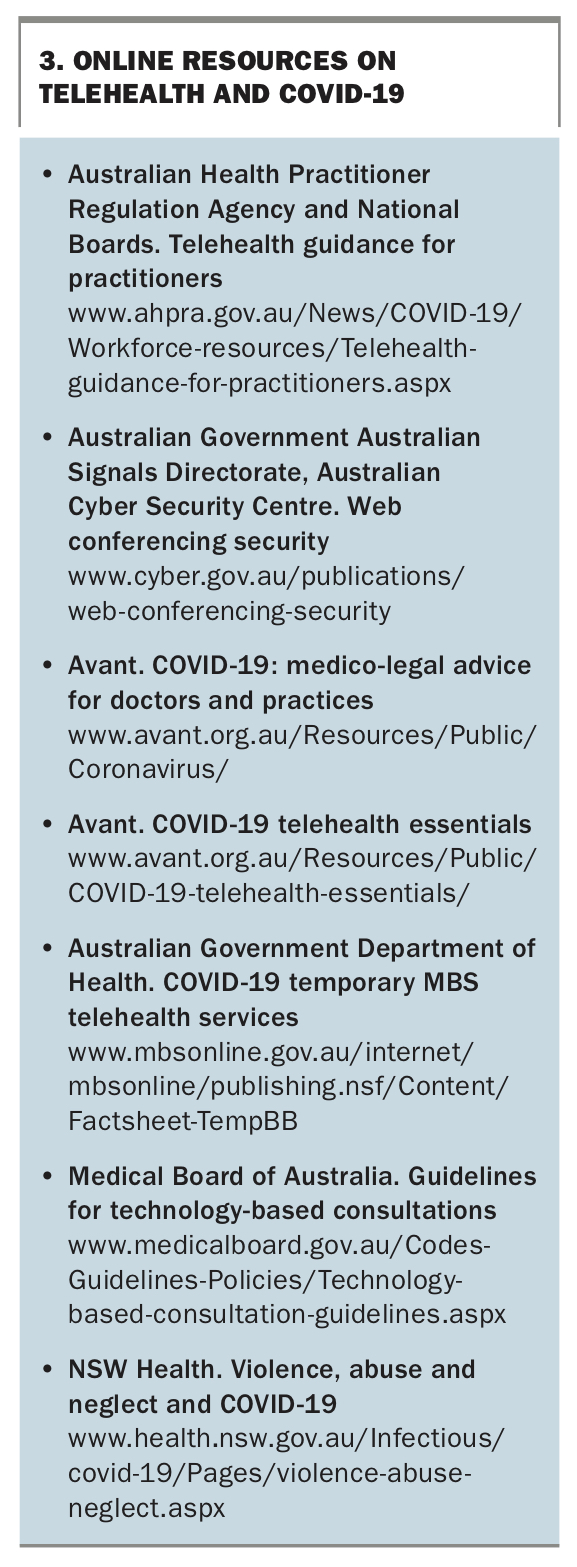
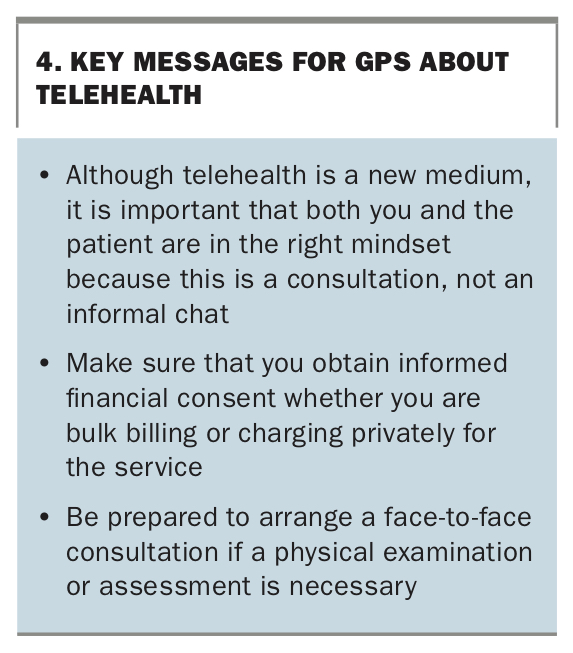
Some useful online resources for medical practitioners on telehealth and COVID-19 are listed in Box 3. Key messages for GPs about telehealth are summarised in Box 4. MT
{kind=link}
{kind=link}
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.