Dyslipidaemia in type 2 diabetes: cardiovascular risk assessment and management

Diabetes type 2
Lipid disorders
GPs play a crucial role in reducing the burden of atherosclerotic cardiovascular disease (ASCVD) in high-risk patients with type 2 diabetes, using a multifactorial approach to risk-factor modification.
- Dyslipidaemia is common in type 2 diabetes and is primarily due to insulin resistance.
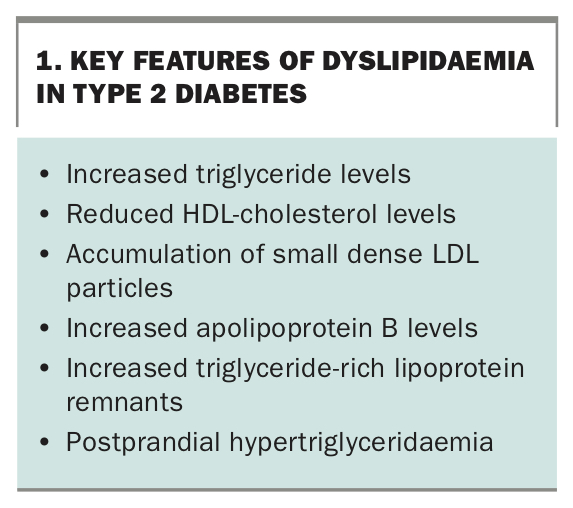
- The typical lipid profile of dyslipidaemia in type 2 diabetes is an increase in triglyceride and apolipoprotein B levels, and a reduction in HDL-cholesterol levels.
- Fasting is not routinely required for measuring the lipid profile, unless triglyceride levels are more than 5 mmol/L in the nonfasting state or a change in therapy is planned.
- Remnant lipoproteins are highly atherogenic triglyceride-rich particles and should be quantitated by calculating non-HDL-cholesterol from the standard lipid profile report; measurement of apolipoprotein B levels is also useful but is not currently Medicare rebatable.
- Glycaemic control, lifestyle factors, obesity, secondary causes of dyslipidaemia and other cardiovascular risk factors should be addressed.
- Risk-enhancing factors may be used to improve cardiovascular risk stratification beyond traditional risk factors.
- Patients with dyslipidaemia and diabetes should be treated with a moderate- or high-intensity statin as first-line therapy to reduce LDL-cholesterol levels.
- Ezetimibe and proprotein convertase subtilisin/kexin type 9 inhibitors should be added to statin therapy if lipid targets are not reached in high-risk patients.
- Fenofibrate should be added to statin and ezetimibe therapy in high-risk patients with optimal LDL-cholesterol levels who remain hypertriglyceridaemic.
Macrovascular disease – atherosclerotic coronary, cerebrovascular and peripheral large artery diseases – is a major complication of type 2 diabetes.1 The pathogenesis of macrovascular disease in diabetes entails a wide spectrum of risk factors, principal amongst which is dyslipidaemia. Dyslipidaemia is common in type 2 diabetes, and may be seen in up to one in three people with the condition.2
This article reviews the pathophysiology, assessment and treatment of dyslipidaemia in people with type 2 diabetes, with a personal perspective based on recent evidence, including international clinical practice guidelines.3-5
How does dyslipidaemia in type 2 diabetes occur?
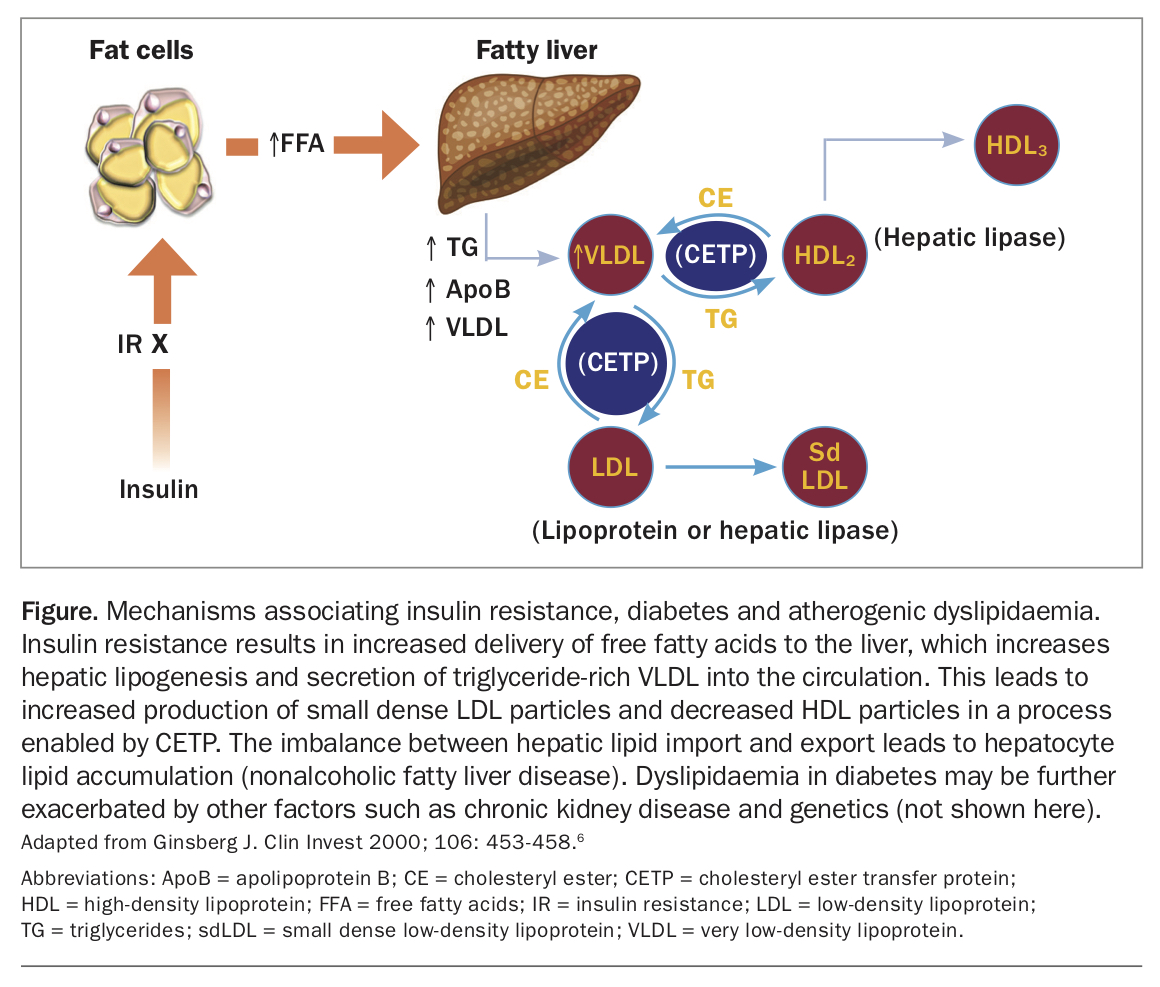
The pathophysiology of dyslipidaemia in type 2 diabetes involves the impact of insulin resistance on peripheral adipose tissue and the liver (Figure).6,7 Insulin resistance is closely related to obesity, present in the vast majority of patients with type 2 diabetes. Insulin resistance results in the increased delivery of free fatty acids from adipose tissue to the liver and upregulation of the hepatic proteins, microsomal transfer protein and apolipoprotein C3, which collectively increase hepatic lipogenesis, leading to increased production and secretion of triglyceride-rich very low-density lipoproteins (VLDL) into the circulation.2,7 This in turn results in increased production of small dense LDL and decreased HDL particles in a process enabled by cholesteryl ester transfer protein.2,7 Insulin resistance also results in an increased production of chylomicron particles in the postprandial state and reduced clearance of triglyceride-rich lipoproteins by the liver.2,7 The atherogenicity of this dyslipidaemia is a consequence of the generation of small dense LDL particles and the accumulation of triglyceride-rich lipoprotein particles in plasma in both the fasting and postprandial state.7
{kind=link}
The plasma lipid profile reflects these changes as an increase in triglyceride and apolipoprotein B (ApoB) levels (reflecting the number of atherogenic lipid particles), as well as by a reduction in HDL-cholesterol (HDL-C) levels (Box 1). An increase in both small dense LDL particles (reflected by an increased ApoB concentration) and triglyceride-rich lipoproteins (reflected by calculated remnant cholesterol or non-HDL-C) are especially atherogenic owing to increased chemical modification in the subendothelial space, uptake by macrophages and retention in the artery wall.7 The toxicity of these lipoproteins is enhanced in diabetes by a coexistent inflammatory, dysglycaemic, hyperoxidative and prothrombotic state. Beyond insulin resistance, dyslipidaemia may be exacerbated by poor glycaemic control, obesity, diet, albuminuria and chronic kidney disease, as well as by medications that disturb lipid and lipoprotein metabolism.
{kind=link}
How to assess?
The plasma lipid profile
The National Vascular Disease Prevention Alliance (NVDPA) 2012 Guidelines for the Management of Absolute Cardiovascular Disease Risk and the RACGP and Diabetes Australia 2016-18 guidelines on General Practice Management of Type 2 Diabetes recommend basing treatment decisions on fasting lipid profiles.8,9 However, elevated nonfasting triglyceride levels are associated with an increased risk of atherosclerotic cardiovascular disease (ASCVD), independent of traditional risk factors.10,11 Recent international guidelines state that fasting is not routinely required for lipid profile measurement, because nonfasting does not lead to a clinically significant difference in total cholesterol, LDL-cholesterol (LDL-C), triglyceride or HDL-C levels compared with a fasting lipid profile in the population.12 However, if triglyceride levels are more than 5.0 mmol/L on a nonfasting lipid profile, these patients should have a repeat sample in a fasting state. In addition, a fasting lipid profile should be performed to assess changes in treatment. When stable, nonfasting lipid profile can be used to monitor treatment over time.
Elevated triglyceride-rich or remnant lipoproteins are more prevalent in patients with type 2 diabetes and are highly atherogenic.11 Measurement of the lipid profile in the nonfasting state also allows the calculation of nonfasting remnant lipoproteins (total cholesterol – HDL-C – LDL-C).12 A nonfasting 1 mmol/L increase of remnant cholesterol is associated with a 2.8-fold increase in the risk of ischaemic heart disease independent of HDL-C.13 Furthermore, the atherogenic risk of remnant lipoproteins can be considered by calculating the remnant lipoproteins, using non-HDL-C (total cholesterol – HDL-C) or by measuring ApoB levels.12 Measurement of ApoB levels has been shown to be the best marker of ASCVD risk, as both LDL-C and triglyceride concentrations become nonsignificant when ApoB was included in a multivariate analysis of the association of LDL-C, triglycerides and ApoB.14 However, although ApoB measurement is available in Australia, it is not currently Medicare reimbursed. Therefore, calculated non-HDL-C may be an appropriate alternative measure for use in general practice.
Cardiovascular risk stratification
People with type 2 diabetes are considered to be at high risk of ASCVD if they are over the age of 60 years, have microalbuminuria (urine albumin:creatinine ratio >2.5 mg/mmol for men and >3.5 mg/mmol for women), moderate chronic kidney disease (persistent proteinuria or estimated glomerular filtration rate [eGFR] <45 mL/min/1.73 m2) or hypertension, according to the NVDPA 2012 guideline.9 In addition, Aboriginal and Torres Strait Islander peoples are considered to be at higher risk.8
The RACGP 2016-18 guideline recommends assessment of ASCVD risk on initial presentation of a patient with type 2 diabetes without established ASCVD, and then assessment and management based on their absolute five-year ASCVD risk (low [<10%], moderate [10 to 15%] or high [>15%]) as assessed by the Australian absolute cardiovascular disease risk calculator (www.cvdcheck.org.au).8 This calculator is based on the Framingham Heart Study and uses total cholesterol and HDL-C as lipid parameters. However, it does not take into account diabetes duration and type, glycaemic control, family history of premature ASCVD or presence of microvascular complications (i.e. albuminuria), all of which affect ASCVD risk. Performing absolute ASCVD risk assessment may also uncover individuals who require specialist assessment for severe or inherited lipid disorders, including those with familial hypercholesterolaemia (who could qualify for Medicare rebated genetic confirmation and treatments), severe hypertriglyceridaemia and chylomicronaemia.
However, international guidelines offer different strategies to cardiovascular risk stratification. The American Heart Association and American College of Cardiology (AHA/ACC) 2018 guideline uses an ASCVD risk calculator called the pooled cohort equation (http://tools.acc.org/ASCVD-Risk-Estimator-Plus/#!/calculate/estimate/) for patients without established ASCVD.5 This risk calculator is not applicable in Australia, as it is not based on studies within the Australian population and it estimates 10-year rather than five-year ASCVD risk. The European Society of Cardiology and European Atherosclerosis Society (ESC/EAS) 2019 guideline offers an alternative method of risk stratification, in which patients with diabetes are either moderate-, high- or very high-risk depending on the presence of ASCVD, target organ damage, additional risk factors, age and duration of diabetes. The ESC/EAS 2019 guideline uses the Systematic Coronary Risk Evaluation (SCORE) calculator to estimate ASCVD mortality; however, the calculator is not recommended in patients with diabetes.4 Using this guideline, no patient with type 2 diabetes is considered to be low risk.4 This approach to risk stratification is simple, includes updated lipid targets and is our preferred approach (see Flowchart 1).
Additional methods of risk stratification
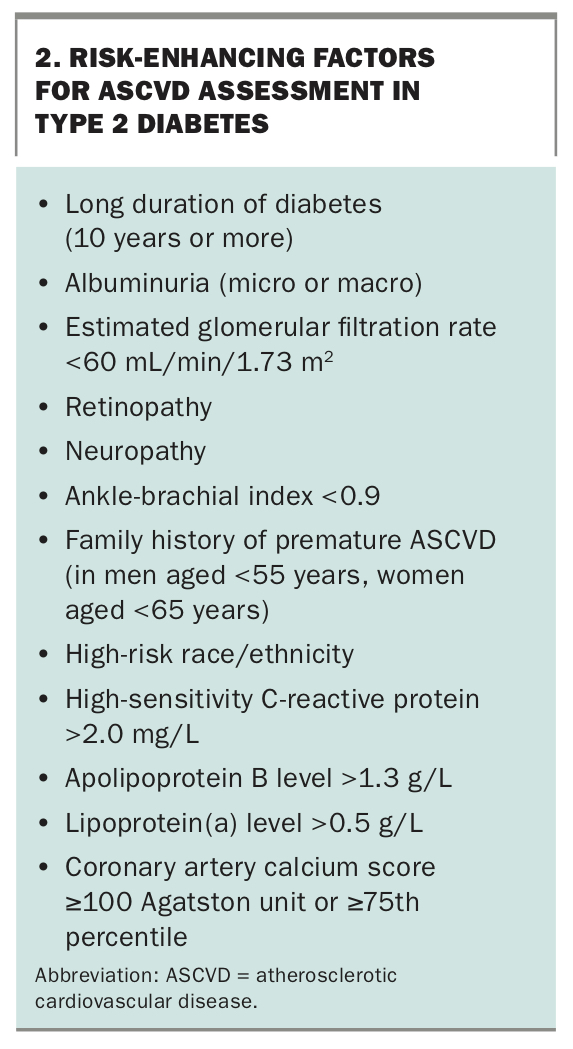
Several risk enhancers may improve ASCVD risk stratification beyond traditional methods. The presence of a risk-enhancing factor according to the AHA/ACC 2018 guideline in patients at low or moderate/intermediate risk favours the initiation of lipid-lowering therapy as these factors can assign patients to a higher risk category (Box 2).5
{kind=link}
Briefly, lipoprotein(a) [Lp(a)] is an LDL-like particle that has an apolipoprotein(a) bound to LDL and is largely genetically determined. Elevated plasma concentrations of Lp(a) predicts ASCVD, peripheral arterial disease and calcific aortic valve stenosis in patients with and without diabetes, independent of other ASCVD risk factors.15-18
In addition, increased coronary artery calcium (CAC) score predicts ASCVD, is superior to risk stratification using traditional risk factors, and can be obtained noninvasively using electrocardiogram-gated noncontrast computed tomography scan.19,20 CAC scoring can be used to identify lower- and higher-risk patients. A CAC score of zero reclassifies patients to a lower-risk group who do not benefit from statin therapy, whereas a score of 100 Agatston units or more, or 75th centile or more for age and sex, is considered higher risk, and statin therapy is recommended.4,5 In patients with type 2 diabetes, evaluation of subclinical atherosclerosis with CAC scoring predicts 10-year coronary heart disease events beyond the Framingham Risk Score and the American pooled cohort equation.20
Measurement of Lp(a) or CAC score may be considered in patients in whom the decision to initiate a statin is uncertain (i.e. low or moderate/intermediate risk); however, these tests are not currently Medicare reimbursed.18 Guidance on these risk stratification methods has been provided elsewhere.18,21
Whom to treat?
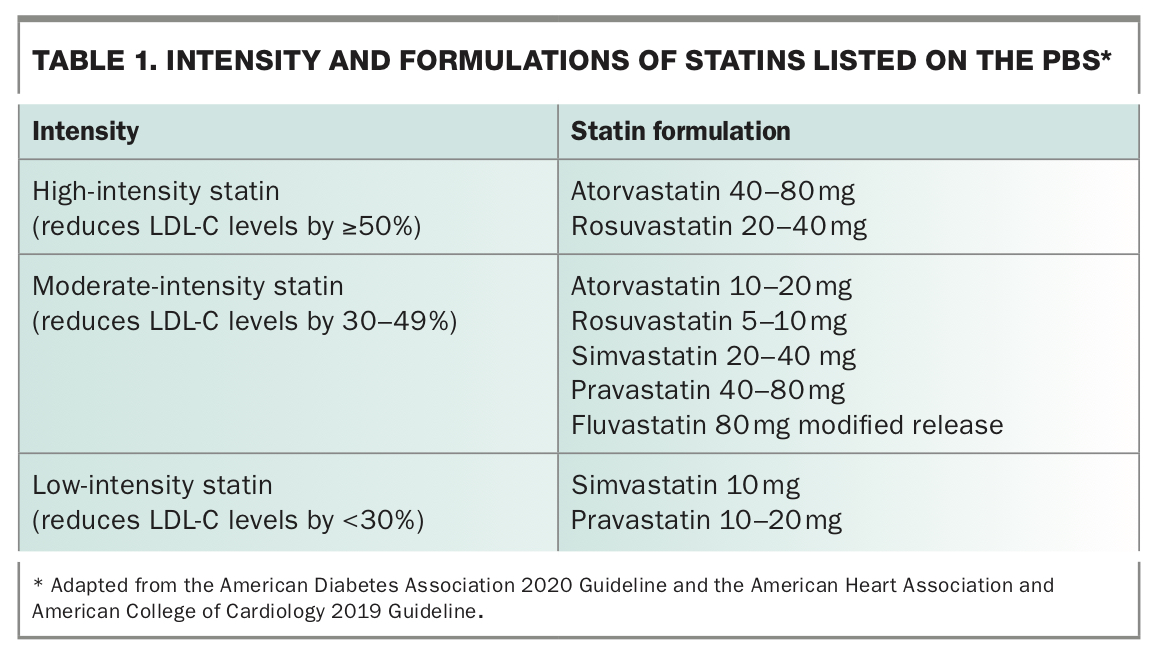
Lowering plasma LDL-C levels using 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitors (statins) decreases ASCVD events in the primary and secondary prevention setting in patients with diabetes.22 Patients with diabetes should be treated with a moderate- or high-intensity statin as first-line therapy rather than a low-intensity statin (Table 1). However, it is important to balance the benefits and potential adverse effects in patients over the age of 75 years.5
{kind=link}
Secondary prevention
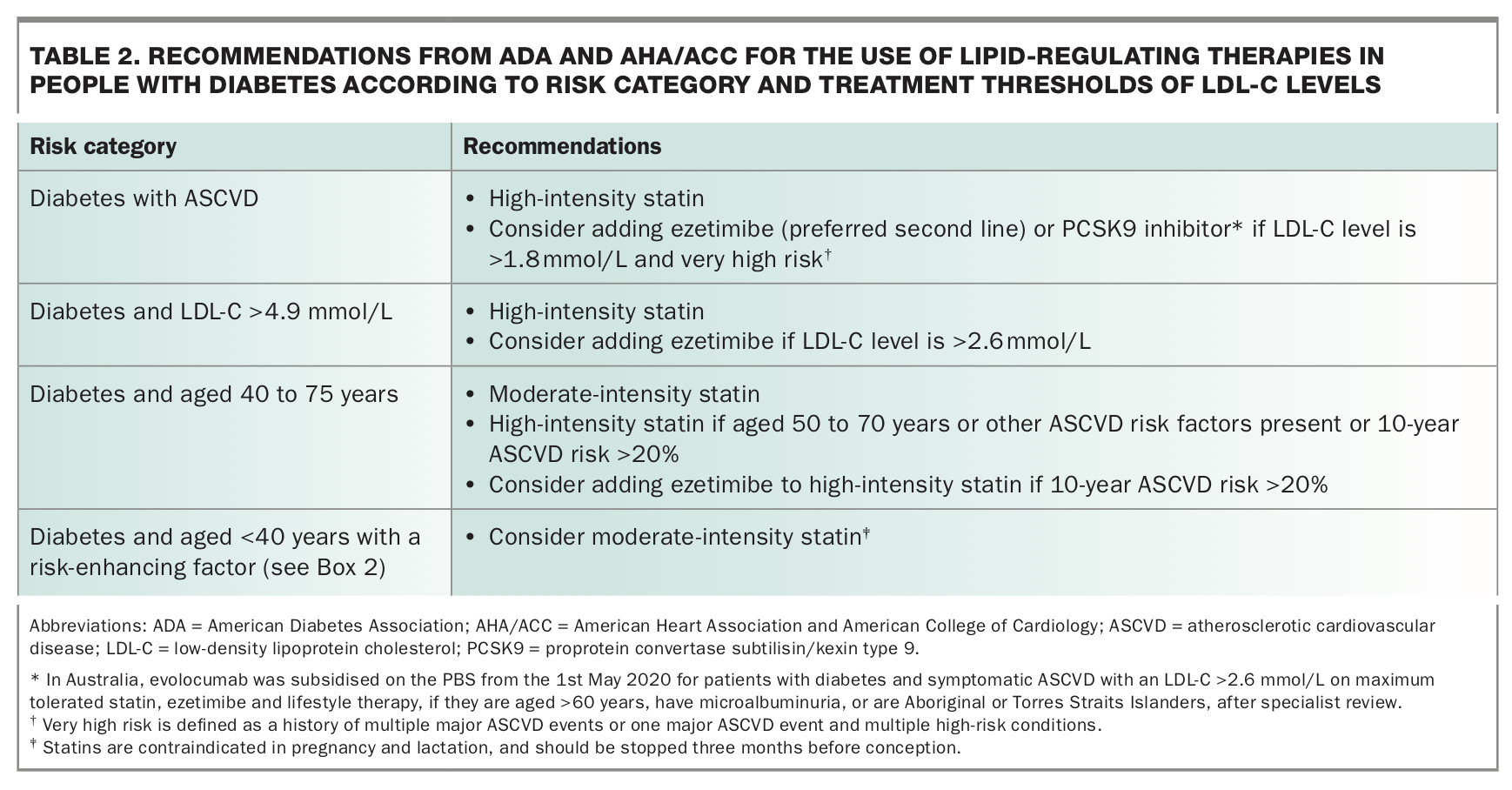
Cholesterol-lowering with high-intensity statin therapy is indicated for patients with diabetes and established ASCVD, irrespective of their lipid levels, acknowledging their significantly increased risk of recurrent events.3,5,23
Primary prevention
According to the RACGP 2016-18 guideline, lipid-lowering therapy is indicated for high-risk patients with type 2 diabetes.8 Lipid-lowering therapy is not routinely recommended unless three to six months of lifestyle intervention has not reduced the risk for patients with type 2 diabetes at moderate (10 to 15%) or low (<10%) five-year ASCVD risk.8 However, if a low- or moderate-risk patient has a risk-enhancing factor based on the AHA/ACC 2018 guideline (Box 2), or is an Aboriginal and Torres Strait Islander patient (RACGP 2016-18 guideline), then lipid-lowering therapy should be considered.5,8
Briefly, the American Diabetes Association (ADA) 2020 guideline and the AHA/ACC 2018 guideline provide different recommendations regarding initiation and intensification of statin therapy based on treatment thresholds (Table 2).3,5 For primary prevention, statin therapy is recommended in people with diabetes over the age of 40 years or who have LDL-C level of 4.9 mmol/L or above (which may suggest familial hypercholesterolaemia).3,5 There is a paucity of data indicating the age at which statin therapy should be initiated, as relatively few patients with type 2 diabetes under the age of 40 years were enrolled in statin trials.22,24 Given the significantly increased life-time risk of developing ASCVD, younger patients with diabetes are likely to benefit from early statin therapy, especially if a risk-enhancing factor is present (Box 2).5,24-26 Statins are contraindicated in women during pregnancy and lactation; they should also be avoided in women planning pregnancy.
{kind=link}
Although aggressive treatment of dyslipidaemia in patients with type 2 diabetes is generally advocated, the large number of guidelines with differing approaches can be confusing.3-5 Our preferred approach is to assess ASCVD risk and use plasma lipid and lipoprotein targets (Flowchart 1) to determine which patient with type 2 diabetes should be initiated on lipid-lowering therapy. This strategy may also guide statin dose titration or use of additional lipid-lowering therapies when targets are not met, enable patient–doctor communication, and facilitate adherence to therapy.4 The NVDPA 2012 guideline also specifies lipid targets, but the targets differ to the ESC/EAS 2019 guideline.4,9 A target driven approach will be further discussed in the next section.
How to treat?
Lifestyle modifications
Patients with diabetes should have individually tailored lifestyle interventions aimed at reducing body weight (by at least 5 to 10%), modifying dietary intake (ideally supported by a dietitian), reducing alcohol intake (≤2 standard drinks per day), increasing physical activity (at least 30 minutes of moderate-intensity physical activity on most, if not all, days) and smoking cessation.8 The Mediterranean diet or the Dietary Approaches to Stop Hypertension (DASH) diet are recommended.27,28
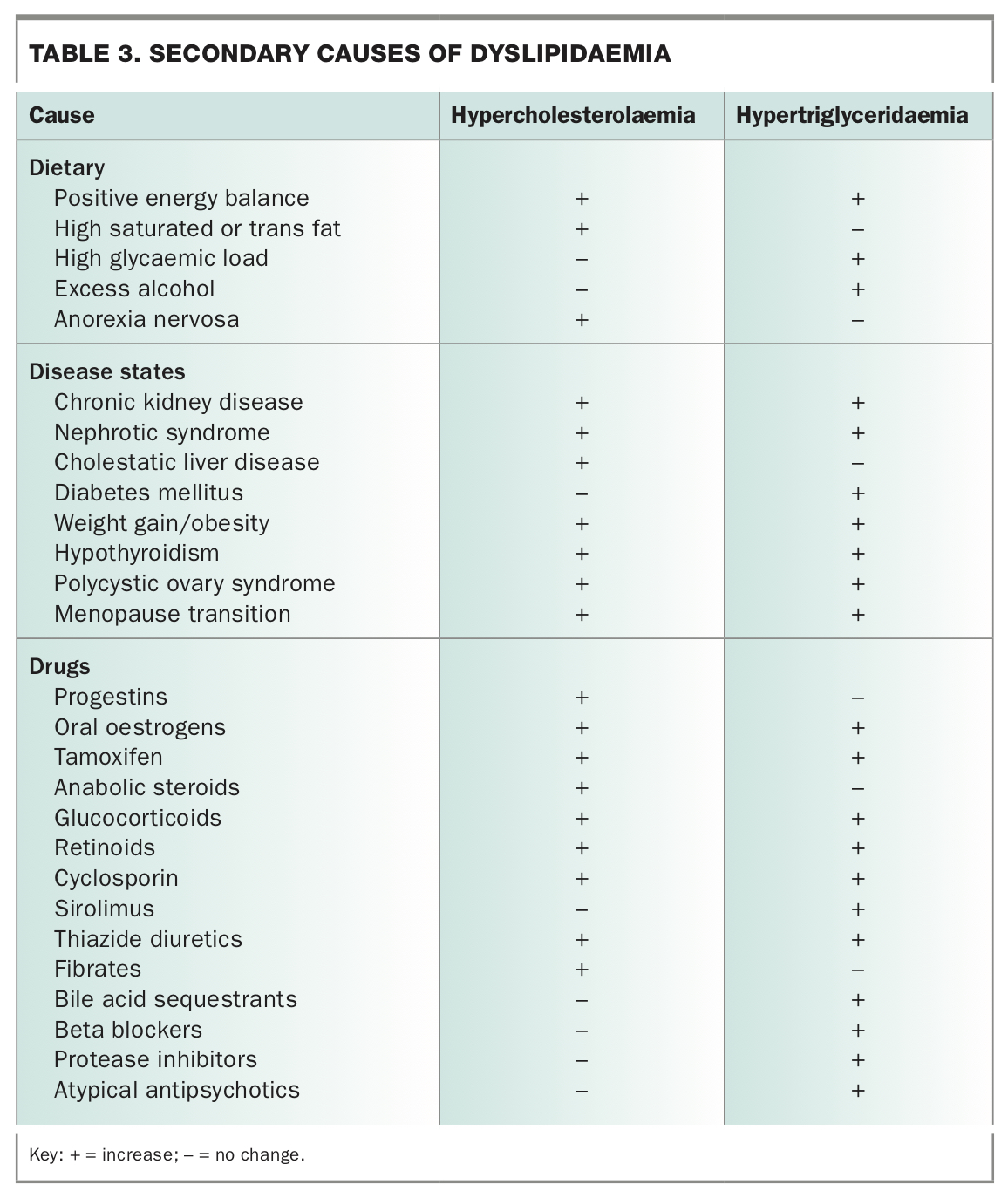
Exclude other causes of dyslipidaemia
Secondary (Table 3) and genetic (primary) causes of the dyslipidaemia (such as familial hypercholesterolaemia, polygenic hypercholesterolaemia, familial combined hyperlipidaemia, familial hypertriglyceridaemia, dysbetalipoproteinaemia and familial chylomicronaemia) should first be identified and treated.29 Optimising glycaemic control and implementing lifestyle modifications can effectively improve dyslipidaemia in type 2 diabetes.
{kind=link}
Reduce LDL-C levels with statin therapy
The first step in managing dyslipidaemia in patients with diabetes is to lower LDL-C levels; therefore, statins are the cornerstone of therapy. The LDL-C targets recommended by the recent ESC/EAS 2019 guideline are presented in Flowchart 1.4 These LDL-C targets are lower than those recommended by previous guidelines, indicating a more intensive approach in modern management.30 High-intensity statins may need to be prescribed at the maximally tolerated dose to achieve these LDL-C targets. The new European guideline also provides ApoB and non-HDL-C secondary targets (Flowchart 1), which are particularly important in patients with type 2 diabetes and hypertriglyceridaemia.4
Reduce LDL-C levels with nonstatin therapies
Nonstatin agents are used when LDL-C targets are not attained despite lifestyle modifications and use of maximally tolerated statins, or as monotherapy in statin-intolerant patients. If LDL-C target is not reached, it is important to assess adherence to statin therapy. The addition of ezetimibe to statin therapy has been shown to reduce LDL-C levels by a further 15 to 30% and lower ASCVD risk, especially in patients with type 2 diabetes and established ASCVD.23,31,32 Furthermore, the addition of proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors, such as evolocumab or alirocumab (both given as subcutaneous injections), to statin therapy has been shown to reduce LDL-C levels by a further 50 to 60% and can lower ASCVD risk, especially in patients with type 2 diabetes and established ASCVD.23,33-36 Ezetimibe is recommended as the second-line agent for lowering LDL-C due to its lower cost. Evolocumab is now subsidised by the PBS after an initial review by a specialist for patients with diabetes and symptomatic ASCVD with an LDL-C of more than 2.6 mmol/L on maximum tolerated statin, ezetimibe and lifestyle therapy, aged over 60 years, have microalbuminuria, or are Aboriginal or Torres Straits Islanders. Trial evidence consistently shows that PCSK9 inhibitors reduce ASCVD risk in high-risk secondary prevention.23,33-36
Bile acid sequestrants, such as cholestyramine, can reduce LDL-C levels, although there is a lack of evidence for reduction in ASCVD outcomes. Additionally, the therapy is often poorly tolerated due to gastrointestinal side effects, decreases the absorption of many drugs, and can be associated with an increase in triglyceride levels.5
Lowering elevated triglyceride levels
Due to the increased ASCVD risk associated with hypertriglyceridaemia, statin therapy should be initiated or intensified to achieve LDL-C and non-HDL-C targets, and lower risk.4 Additional therapies may be required in patients with hypertriglyericidaemia because statins reduce triglyceride levels by only 10 to 20%.4 Although there are no specific triglyceride or HDL-C treatment targets in the ESC/EAS 2019 guideline, this guideline did specify non-HDL-C and ApoB targets (Flowchart 1),4 which are particularly applicable to patients with diabetes.
In the overall group of patients enrolled in clinical endpoint trials, the combination of statin plus a fibrate has not been shown to reduce ASCVD risk.37,38 Accordingly, this combination is not recommended by the ADA 2020 guideline or ACC/AHA 2018 guideline.3,5 However, the ESC/EAS 2019 guideline recommends consideration of combination therapy when LDL-C is at target but triglyceride level is 2.3 mmol/L or above (Flowchart 2), as prespecified subgroup analyses and meta-analyses have shown ASCVD benefit with fibrates in moderate hypertriglyceridaemia.4,39,40 Fenofibrate is preferred over gemfibrozil, owing to the lower risk of myopathy when used in combination with statin therapy.5 Fenofibrate can also reduce the progression of retinopathy in patients with type 2 diabetes and pre-existing retinopathy, irrespective of baseline lipid levels, and is approved for this indication in Australia.38,41 In patients with severe hypertriglyceridaemia (fasting triglyceride levels of 5.6 mmol/L or more), fibrate or fish oils should be considered to reduce the risk of acute pancreatitis.3,5
Statin plus niacin combination therapy has also not been shown to reduce ASCVD risk, and is associated with increased adverse effects.38,42 This combination is also not routinely recommended for reducing ASCVD risk.3-5
Icosapent ethyl, a highly purified ethyl ester of eicosapentaenoic acid, at 4 g/day, has been shown to reduce ASCVD risk in high-risk patients with fasting triglyceride levels between 1.5 and 5.6 mmol/L who are on statin therapy.43 At present, icosapent ethyl is not registered for use in Australia, and the results of the icosapent ethyl trial should strictly not be extrapolated to other omega-3 fatty acid products. In the US, icosapent ethyl is branded as Vascepa, which has recently come off-patent, therefore, generic formulations may potentially become available in Australia in the near future.
Statin-associated side effects
Statins are generally well tolerated and side effects were rare in trials. However, there is a general public perception that statin use results in side effects, fuelling the nocebo effect.44 Adequately addressing the benefits and risks of statins may improve adherence. Strategies including rechallenging with a lower dose, alternate-day dosing or trialling an alternative statin should be considered for patients who do not tolerate the intended dose of a statin. Evaluation of other causes of muscle symptoms or factors predisposing to statin side effects must be undertaken.5 If statin-associated muscle symptoms are severe, rhabdomyolysis should be considered and creatinine kinase level measured. The management of statin intolerance has been reviewed elsewhere in detail.45
Conclusion
Dyslipidaemia in type 2 diabetes is characterised by a cluster of lipid and lipoprotein abnormalities that are primarily secondary to insulin resistance and result in accelerated macrovascular disease.
Informed by recent major international guidelines that have a common base, we have provided our opinion on the optimal approach to ASCVD risk assessment, setting of lipid targets and use of statin and nonstatin therapies for dyslipidaemia in patients with diabetes. GPs encounter many high-risk patients with type 2 diabetes and play a crucial role in reducing the burden of ASCVD based on a multifactorial approach to risk-factor modification.46 MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.