Reducing cardiovascular risk in type 2 diabetes: emerging therapies

Diabetes type 2
Lipid disorders
The increased risk of developing atherosclerotic cardiovascular (CV) diseases in people with type 2 diabetes is well recognised, and a focus on reducing CV risk is just as important as glycaemic control. An individualised multifactorial approach to treating patients with type 2 diabetes is recommended, including lifestyle modification and drug therapy to reduce CV risk and improve renal outcomes, blood pressure control, and lipid and glucose levels.
People with type 2 diabetes mellitus are at higher risk of developing atherosclerotic cardiovascular diseases (ASCVDs) than those without diabetes.1,2 Optimal management of type 2 diabetes and associated CV risk factors is recommended to address the increased risk of CV and related diseases.3 Until recently, drug therapy for treating elevated blood glucose levels has had little, if any, impact on reducing ASCVD and its complications in people with type 2 diabetes; however, new glucose-lowering therapies have shown promising results in reducing CV risk. This review will examine the multifactorial approach to reducing CV risk in people with type 2 diabetes, specifically examining the role of the newer glucose-lowering agents that have become available over the past few years.
Multifactorial CV risk reduction in type 2 diabetes mellitus
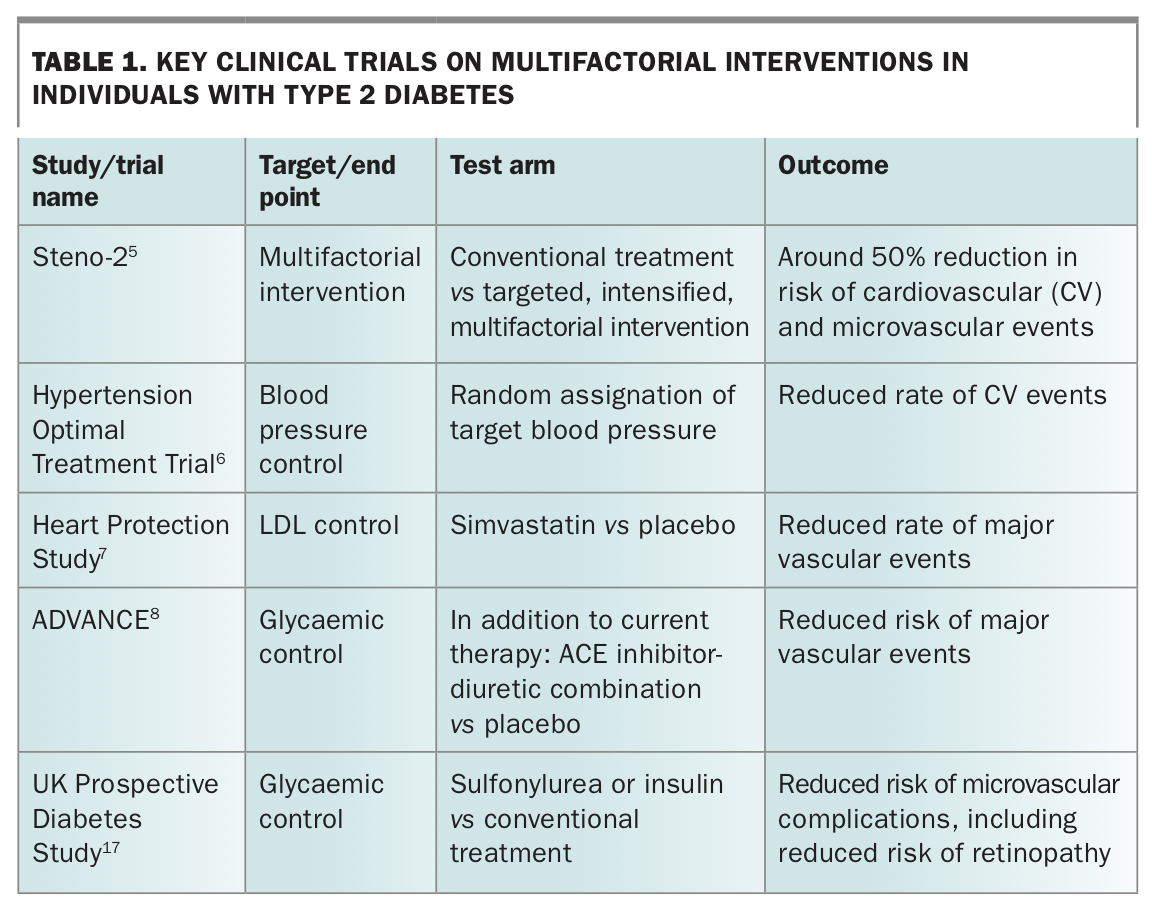
In the past, many medical practitioners have had a glucocentric approach to managing type 2 diabetes, focusing primarily on controlling hyperglycaemia and preventing hypoglycaemia, of which the latter is associated with an increased risk of cardiac events.4 CV disease is prevalent in people with type 2 diabetes and responsible for more morbidity and mortality than the complications of diabetes itself; therefore, slowing and reducing the development of vascular disease and subsequent CV events should be of equal or greater importance to glycaemic control in the management of type 2 diabetes. The Steno-2 study reinforced that a multifactorial approach to modifying risk factors (such as reducing blood pressure and lipid and glucose levels) reduced both macrovascular and microvascular complications in individuals with type 2 diabetes.5 Both the Hypertension Optimal Treatment Trial and the Heart Protection Study showed significant reductions in CV events in individuals with type 2 diabetes, based on a reduction in diastolic blood pressure and LDL level, respectively.6,7 Several other studies have also demonstrated positive CV outcomes associated with reduced blood pressure in patients with type 2 diabetes.8,9 These studies are discussed below and summarised in Table 1.
{kind=link}
Blood pressure control
There is no single target blood pressure that should be aimed for in people with diabetes; diabetes management guidelines, including those from the Royal Australian College of General Practitioners and Diabetes Australia, recommend systolic and diastolic targets of below 140 and 90 mmHg, respectively, as a guide to treatment, but below 130/80 mmHg if significant proteinuria exists (timed overnight collection: above 20 mcg/min or spot collection above
20 mg/L).3,10,11 Therefore, treatment target levels should be individualised for all patients, taking other comorbidities into account.3 Renin-angiotensin-aldosterone system blockers, ACE inhibitors or angiotensin-receptor blockers are usually the first choice for treating hypertension in people with type 2 diabetes, especially in the presence of albuminuria, followed by the addition of dihydropyridine calcium channel blockers, a combination that has shown significantly better outcomes than ACE inhibitors in combination with thiazide diuretics.10-12
Lipid control
The target LDL cholesterol level should be the same for individuals with type 2 diabetes and those with established CV disease (i.e. below 1.8 mmol/L), as type 2 diabetes is often referred to as a coronary risk equivalent.3 However, recently published data show that lowering LDL cholesterol level even further (below 1.4 mmol/L) is associated with greater risk reduction, especially in patients with established ASCVD.13,14
Glycaemic control
Lowering glycated haemoglobin levels in people with type 2 diabetes has been shown to reduce CV and renal disease, with most of these benefits reducing microvascular events.15,16 Intensifying glucose-lowering therapy results in a reduction in microvascular complications, both retinal and renal. The UK Prospective Diabetes Study showed reduced risk of retinopathy in patients with newly diagnosed type 2 diabetes assigned therapy with sulfonylureas or insulin compared with those assigned metformin.17,18 The ADVANCE study showed that more intensive glycaemic control improved renal outcomes, especially with respect to development or progression of nephropathy.8 Most clinical trials over the past two decades, as well as a meta-analysis, have failed to demonstrate clear benefits of glucose-lowering therapies on various CV endpoints, which is disappointing given ASCVD is the major cause of morbidity and mortality in people with type 2 diabetes.19-22
New glucose-lowering therapies and CV risk reduction
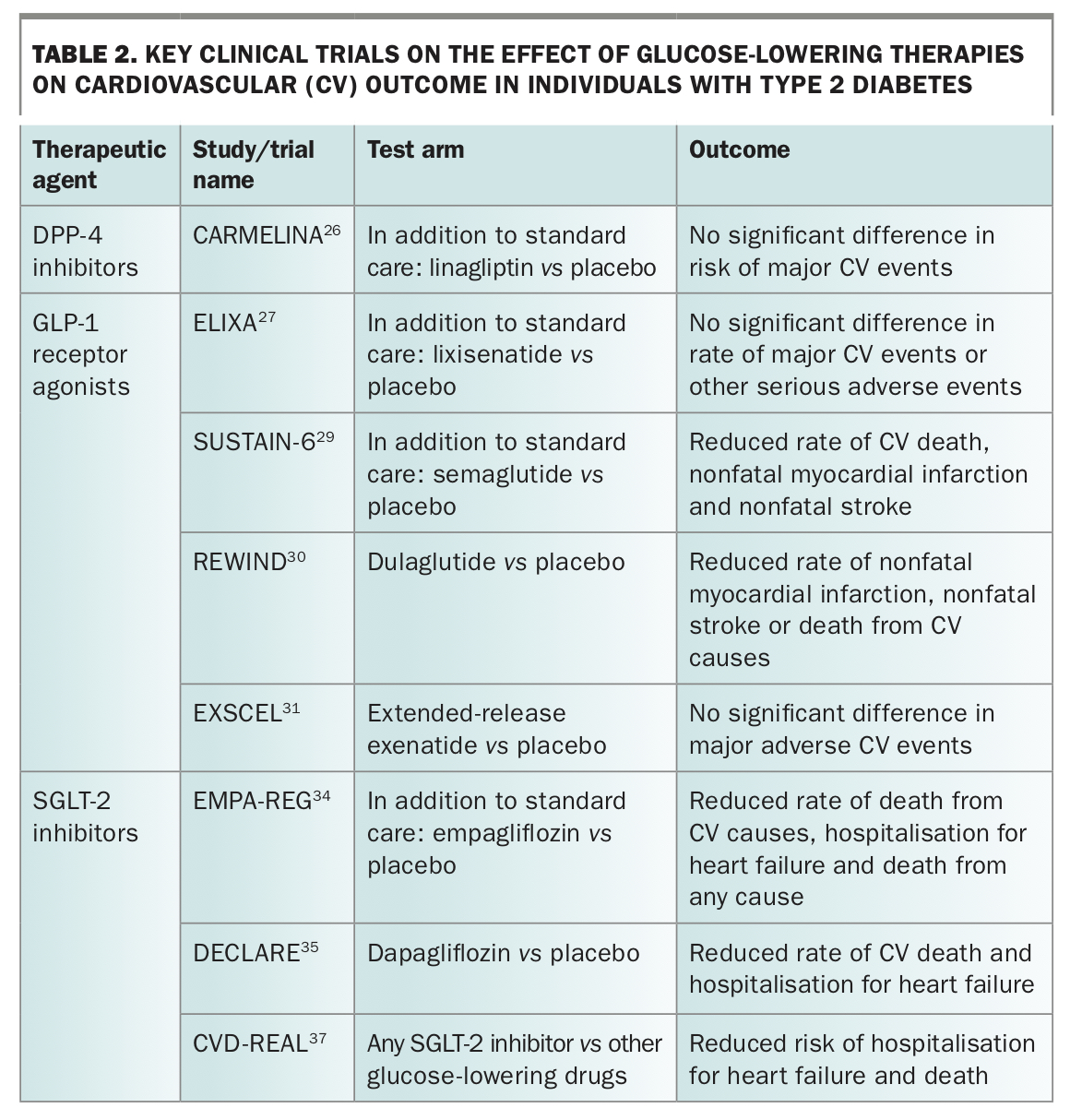
Recently, three classes of therapeutic agents have emerged as possible new treatments in reducing the risk of CV events in people with type 2 diabetes: dipeptidyl peptidase 4 (DPP-4) inhibitors, glucagon-like peptide-1 (GLP-1) agonists and sodium glucose cotransporter-2 (SGLT-2) inhibitors. The results of key clinical trials are discussed below and summarised in Table 2.
{kind=link}
DPP- 4 inhibitors
The DPP-4 inhibitors (saxagliptin, alogliptin, sitagliptin and linagliptin) have been extensively studied in people with type 2 diabetes and high CV risk and were found to be neutral with respect to CV events (myocardial infarction, stroke and CV death).23-26 There was an increased risk of hospitalisation for heart failure (HF) with saxagliptin and a trend to this with alogliptin, so these agents should be used cautiously in patients with a history of HF. DPP-4 inhibitors have an important role in glycaemic control and are well tolerated with minimal side effects, but have no benefit in reducing CV events in people with type 2 diabetes.
GLP-1 receptor agonists
The GLP-1 receptor agonists have shown mixed results in their effects on reducing CV risk. Lixisenatide has shown neutral CV effects when assessed in people with type 2 diabetes after acute coronary syndrome, whereas liraglutide, semaglutide and dulaglutide significantly improved CV outcomes in people with type 2 diabetes at high CV risk.27-30 Additionally, the EXSCEL study reported a potential CV benefit of the long-acting, once-weekly GLP-1 analogue, exenatide (extended-release), although the primary endpoint did not reach statistical significance (p=0.06).31 Interestingly, although there was a significant decrease in all-cause mortality for the overall study group in the EXSCEL trial, post-hoc subgroup analysis showed that patients with peripheral arterial disease had worse outcomes on study medication.32
GLP-1 receptor agonists also have a renal protective effect but no effect on development of HF. These injectable agents are often associated with significant weight loss, independent of the nausea they often cause, by promoting earlier satiety, delaying gastric emptying and suppressing appetite. They are injectable, so some patients are not enthusiastic about using them, but once-weekly treatment is generally acceptable.
SGLT-2 inhibitors
The introduction of the SGLT-2 inhibitors (empagliflozin, dapagliflozin and ertugliflozin) has changed the landscape of type 2 diabetes treatment. Significant CV and renal benefits have been seen in patients with and without pre-existing ASCVD in studies when empagliflozin and dapagliflozin have been compared with placebo.33-35 The CV and renal benefits of ertugliflozin are consistent with those seen from other SGLT-2 inhibitors.36 These agents promote glycosuria by blocking the SGLT-2 receptor in the renal tubules, resulting in reduced CV risk factors including blood glucose levels, body weight and blood pressure.33 In the EMPA-REG study, patients with established ASCVD who were assigned to empagliflozin in addition to standard care had reduced CV events, CV and all-cause mortality and HF, as well as improved renal protection compared with patients assigned to placebo.34 In the DECLARE study, patients with and without established ASCVD were assigned to either dapagliflozin or placebo. The study showed a reduced rate of hospitalisation for heart failure and increased renal protection in patients treated with SGLT-2 inhibitor compared with the placebo group; however, a reduction in CV events was not shown.35 Real-world data from a very large observational study (CVD-REAL), conducted in clinical practice in the US and Europe, supported the CV benefits of the SGLT-2 inhibitors reported in these randomised trials.37
The effects of SGLT-2 inhibitors on CV event and HF reduction and renal protection in these studies are disproportionate to the changes in glycated haemoglobin level, body weight and blood pressure seen with their use, suggesting that mechanisms independent of these changes are involved in CV and renal outcomes. These mechanisms have not yet been definitively defined but effects on myocardial energy metabolism, renal tubule-glomerular feedback and the use of ketones as a fuel substrate may be involved. There is also emerging evidence that SGLT-2 inhibitors affect the sodium/hydrogen exchanger at a cellular level, which increases mitochondrial ATP and thus energy production.38
Given the reduction in CV events and death in patients who have established CV disease with empagliflozin use, and the renal protection and reduction in HF with all SGLT-2 inhibitors in patients with type 2 diabetes with and without established CV disease, SGLT-2 inhibitors should be considered in most patients with type 2 diabetes. Care must be taken, however, as there is an increased risk of fungal genital and urinary tract infection, and, rarely, Fournier’s gangrene due to glycosuria. Good genital hygiene is therefore essential if they are used. Additionally, if a patient becomes unwell and cannot maintain their oral fluid intake, or requires fasting for a procedure, it is essential that SGLT-2 inhibitors be transiently discontinued to avoid the risk of euglycaemic diabetic ketoacidosis.
Conclusion
ASCVD is the major cause of morbidity and mortality in people with type 2 diabetes, and CV risk reduction is as important as glycaemic control in the treatment of these patients. Recent studies with newer agents have shown that CV events, mortality, HF and renal protection can be improved with these new therapies, but the choice of therapy still needs to be individualised according to patient characteristics. It remains extremely important to control blood pressure and lipid and blood glucose levels in these patients, and therapeutic agents are now available that have both glycaemic and cardiorenal benefits when used to treat people with type 2 diabetes. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.