Strabismus: what GPs need to know

Strabismus is a common disorder in children and adults that is often perceived as complicated and perplexing. Assessment and management of strabismus can be simplified through an understanding of the common conditions and patterns of presentation.
Strabismus, also known as ‘squint’, is a misalignment of the visual axes of the two eyes. It is a common disorder, with a prevalence of 3% in children and adults.1 Esotropia is a convergent misalignment where the eyes cross inward. A divergent misalignment, where one or both eyes look outward, is known as exotropia. The prevalence of strabismus varies by ethnic background, with esotropia more common in western populations and exotropia more common in Asians.2
Early-onset strabismus, presenting in the first 2 years of life, is associated with impaired development of binocular vision, as well as amblyopia (‘lazy eye’). Acquired strabismus in older children, from about the age of 5 years, and adults can result in troublesome double vision (diplopia). However, several treatment options with high rates of success are available for strabismus. The underlying cause of the patient’s strabismus will guide treatment. Common causes are shown in Table 1 for children and Table 2 for adults. An understanding of the six extraocular muscles and their primary actions (Figure 1) is also helpful in diagnosing types of strabismus that relate to the cranial nerves or particular eye muscles. GPs have a crucial role in assessing patients presenting with symptoms of strabismus and referring them for a complete assessment in a specialised ophthalmology clinic.
{kind=link}
{kind=link}
{kind=link}
Symptoms and complications of strabismus
In adults, intermittent or constant strabismus may cause troublesome symptoms with vision, such as:
- double vision, where an object will be seen to be in two different places
- visual confusion, where two separate objects appear to be superimposed
- reduced field of vision, secondary to esotropia or restrictive strabismus, in which there is a limitation of eye movements.
Patients can also experience a negative psychosocial impact because of an abnormal appearance. This can significantly affect their daily social interactions, with studies showing that patients with strabismus have a reduced quality of life.3
In childhood, constant strabismus leads to loss of binocular function. Children adapt to strabismus to avoid double vision or visual confusion by suppressing the image from one eye at the cortical level. In a child younger than 5 years, a strabismus that does not alternate equally between the two eyes may lead to one eye developing amblyopia.
Strabismus can also be a contributing factor to poor motor co-ordination and negative psychosocial development.4 If the child needs to adopt an abnormal face posture to retain binocular vision, this can lead to musculoskeletal problems and facial asymmetry.
Evaluation of strabismus in general practice
A careful history and examination of a patient presenting with symptoms of strabismus will usually lead to the correct diagnosis. It is important to remember that poor vision (sensory strabismus), myasthenia gravis and temporal arteritis may present with almost any pattern of strabismus.
History
History taking should include the presence and time course of symptoms, ocular and medical history, any family history of strabismus and the patient’s social history, including their occupation and driving status.
Symptoms include monocular or binocular double vision, asthenopia (eye strain) in patients with intermittent or decompensating strabismus and an abnormal appearance of the eyes. If the patient has monocular double vision (symptomatic with only one eye open), other causes not related to strabismus, such as cataract, astigmatism or macular abnormalities, need to be considered. For patients with double vision, an assessment should be made of whether the two images are horizontally, vertically or obliquely displaced.
Symptoms may be intermittent or constant. Sudden onset of symptoms likely indicates a vascular abnormality, whereas gradual onset indicates decompensation of an underlying strabismus from childhood or a compressive lesion. If strabismus symptoms are variable (with changing pattern and severity) and fatiguable (worse when tired, unwell or at the end of the day), myasthenia gravis should be considered.
Ocular history includes any strabismus, eye patching or wearing of glasses as a child, as well as any history of strabismus surgery. Relevant medical history includes neurological symptoms, such as headache, weakness or tinnitus; trauma, neurological disease or thyroid abnormalities; and vascular risk factors for ischaemic cranial neuropathy.
Examination
Examination should include assessment of best corrected visual acuity, acquired head posture, ocular alignment, eye movements of each eye, pupil examination and eyelid position.
Testing of best corrected visual acuity is important to assess for amblyopia and a potential sensory cause of strabismus. In adults, visual acuity assessment is performed monocularly using a distance Snellen chart. Age-appropriate methods, such as the fix and follow test or forced preferential looking test, should be used for children.5
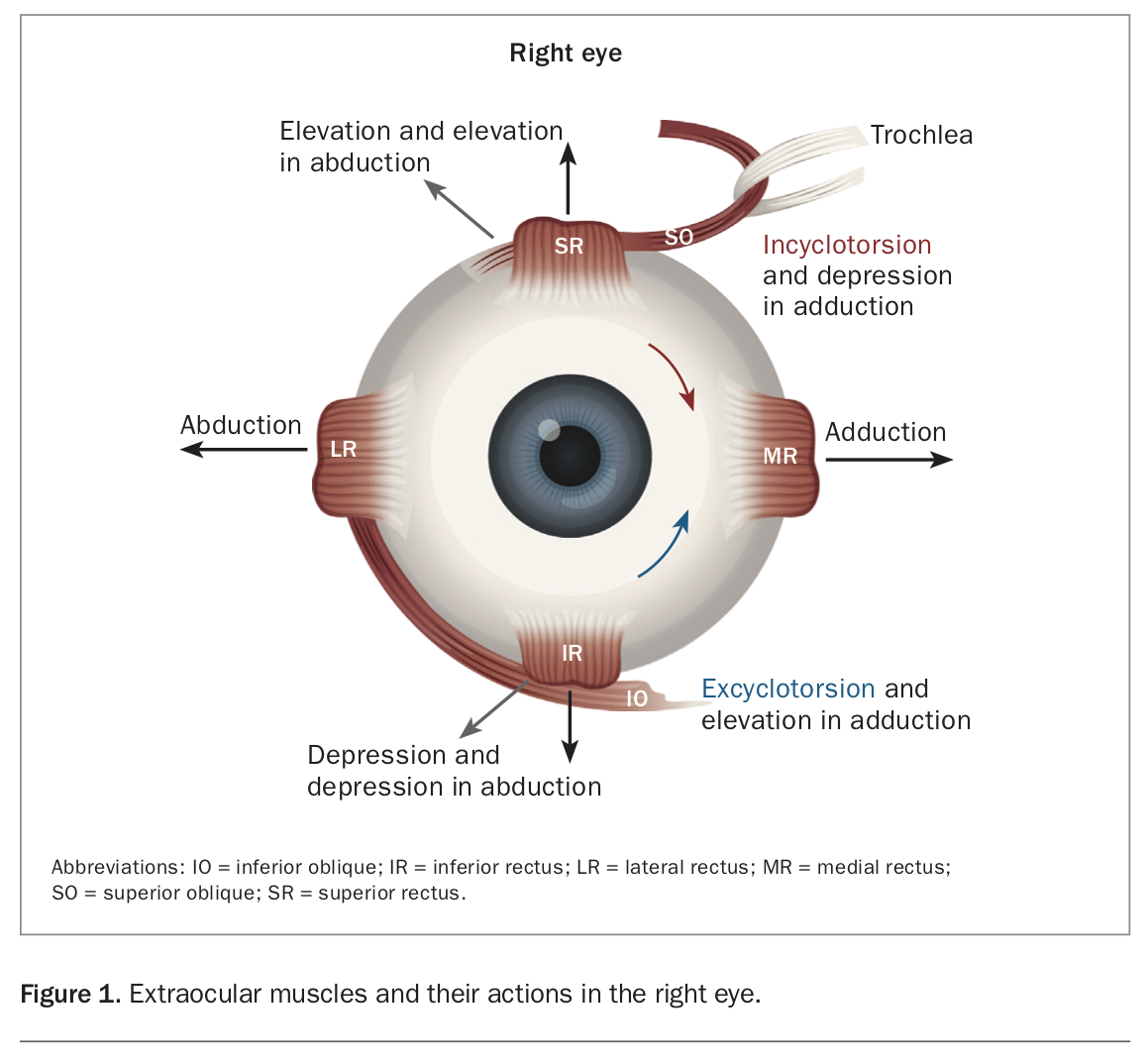
Patients with strabismus may adopt an acquired head posture to help them maintain single vision. For example, patients with a lateral rectus palsy will turn their head to the affected side (Figure 2a).
{kind=link}
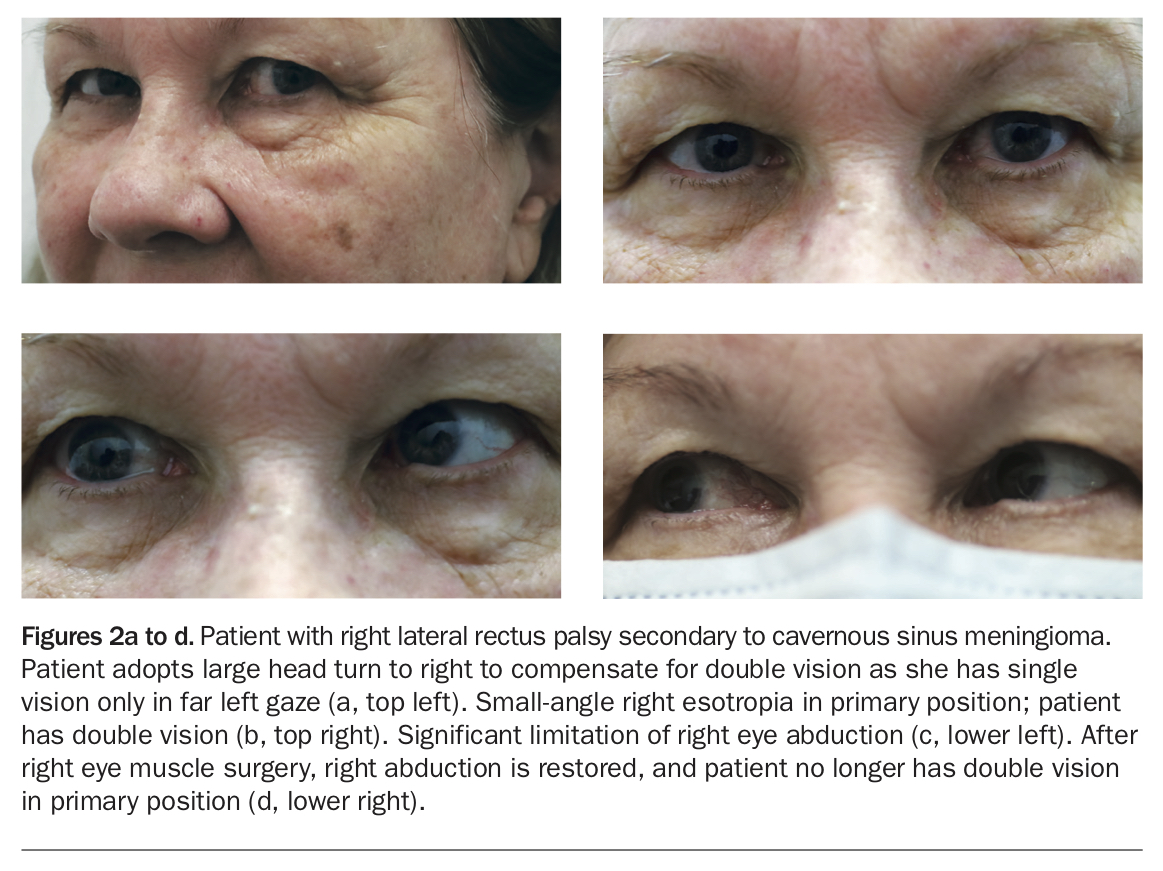
Cover testing is used to test ocular alignment. The patient is asked to fixate on a distant target, and each eye is occluded independently to assess whether the uncovered eye makes a refixating movement (Figure 3). If no movement is seen in either eye, there is no manifest strabismus, also known as a tropia. A latent strabismus, or phoria, is detected by alternately covering one eye, then the other, so that the fusional mechanisms that control alignment are disrupted. In a young child, assessing the symmetry of corneal reflexes with the Hirschberg test is helpful to test ocular alignment.5
{kind=link}
Eye movements are tested by asking the patient to follow a light to the extremes of gaze in an ‘H’ pattern. It is important to test eye movements for each eye separately, with the other eye being occluded. In patients with strabismus, eye movements may appear to be limited if tested with both eyes open, depending on which eye is the fixating eye. Any true limitation of eye movement would suggest a cranial nerve palsy or restrictive abnormality (e.g. orbital floor fracture or thyroid orbitopathy).
A dilated pupil in a patient with new exotropia or hypotropia (where one eye is lower than the other) would suggest oculomotor palsy. Ptosis, or drooping, of the eyelid would also suggest oculomotor palsy or myasthenia gravis.
Investigations
Appropriate investigations depend on the differential diagnosis from the clinical assessment. When decompensation of childhood strabismus is suspected, an old family photo album may show a small misalignment or an abnormal head posture in the patient as a child. Testing of antibodies for myasthenia gravis may be ordered in patients with variable strabismus, especially if there is ptosis and fatiguability. A new-onset cranial neuropathy requires a complete neurological examination and urgent neuroimaging in most cases. Temporal arteritis must be considered in any patient over the age of 50 years with new-onset cranial neuropathy.
Red flags
Urgent ophthalmological review and MRI of the brain are recommended to exclude acute intracranial abnormalities when:
- a child or adult has sudden-onset constant strabismus
- strabismus is associated with new reduced vision, headache or focal neurological signs
- a child presents with true binocular double vision (primary strabismus disorders of infancy are not associated with double vision because of cortical suppression of the deviated eye)
- strabismus is associated with anisocoria (where one pupil is a different size to the other) or ptosis, in which case oculomotor palsy needs to be excluded.
When to refer
Most children and adults with strabismus would benefit from referral to an ophthalmologist with an interest in the disorder. This would facilitate a detailed ocular motility assessment, often in conjunction with an orthoptist, and provide the full range of management options.
The urgency of referral should be based on the age of the patient and the suspicion of acute abnormality. Infants and young children should be seen sooner to facilitate prompt treatment of potential amblyopia and abnormal binocular vision.
Management of strabismus
Observation is appropriate management if there are no functional or psychosocial consequences of the strabismus. Beyond this, there are various treatment options available. The best treatment option will depend on several factors, including the patient’s symptoms, age, underlying diagnosis and previous treatment. Any reversible disease process (e.g. cataract or Graves’ disease) needs to be managed appropriately.
Glasses
Glasses may be prescribed for many reasons for a patient with strabismus. Improving a patient’s vision can improve the central fusion of the images from the two eyes and therefore keep the eyes better aligned. In some conditions, such as accommodative esotropia, where the convergence arises from long-sightedness, relieving the long-sightedness with full-time wearing of glasses can be partially or completely curative. Children with secondary or concurrent amblyopia would usually need patching of the better-seeing eye in addition to glasses.5
Prisms
Prisms can be used to treat double vision by shifting the image seen through one or both eyes and compensating for the ocular misalignment. They are particularly useful for small-angle and comitant strabismus, in which the angle of strabismus is similar in different positions of gaze (e.g. age-related distance esotropia). Temporary Fresnel prism can be applied onto the patient’s existing glasses as a trial treatment; if the patient’s symptoms are well controlled, the prism can then be ‘ground in’ to lenses by the optician.
Occlusion
Occlusion is used for symptomatic relief of double vision in adults where prism correction is not possible. Occlusion of one eye can be achieved through a patch on the skin or over the glasses frame. An opaque contact lens is a more cosmetically acceptable form of occlusion and may be suitable for some adults. In children with acquired strabismus (e.g. a cranial nerve palsy), alternating occlusion of both eyes may be prescribed temporarily to reduce the risk of strabismic amblyopia. Adults with constant double vision should have occlusion until definitive assessment and management can be offered. These patients should not drive for at least three months while adapting to monocular viewing.
Orthoptic exercises
Eye exercises to improve fusional mechanisms and binocular function are taught by trained orthoptists and can be carried out by patients at home. They can be beneficial in treating symptomatic convergence insufficiency, which is the inability to sustain binocular function when focusing on near objects (e.g. reading).
Pharmacological treatments
Pharmacological treatments with botulinum toxin or bupivacaine injections aim to weaken or strengthen extraocular muscles by minimally invasive, nonsurgical means. For example, botulinum toxin can be injected directly into an extraocular muscle to induce temporary paralysis. It is used in the treatment of strabismus when surgery is contraindicated or in situations where future improvement is predicted (e.g. microvascular cranial nerve palsy).
Eye muscle surgery
Eye muscle surgery involves permanently weakening, strengthening or moving extraocular muscles. Surgery is not a final or last-resort treatment for strabismus and, in many cases, it may be the best or only suitable option. Eye muscle surgery to restore appropriate ocular alignment may be indicated for functional or reconstructive purposes. Functional indications include restoring single vision or normal head posture. Surgery can be undertaken on one or both eyes, and the surgical plan depends on the size and pattern of strabismus, as well as the underlying diagnosis. It is a day procedure and routinely performed under general anaesthesia for both children and adults, after the patient’s fitness for general anaesthesia has been assessed in conjunction with their GP or paediatrician and other physicians. Antiplatelet and anticoagulant medications are not stopped perioperatively.
Surgical results may be improved by the use of adjustable sutures, a technique that allows for fine-tuning of the muscle position after the patient recovers from general anaesthesia. This can be particularly helpful in cases where the outcome is less predictable, such as reoperations and in patients who are at risk of postoperative double vision. In suitable patients, the adjustment is performed under topical anaesthesia, generally within the first 24 hours after surgery.
Recovery from strabismus surgery is usually fairly rapid, with most children and adults returning to normal activities in a few days. Simple oral analgesia and cool compresses are helpful in the immediate postoperative period. Patients are advised not to swim for at least two weeks. A combination of corticosteroid and antibiotic drops is usually prescribed for one to two weeks.
Clinical scenarios
A child with intermittent strabismus noticed by parents
Childhood strabismus is often initially observed by parents or caregivers as intermittent deviations seen in photos and when the child is tired or unwell. Common diagnoses to consider are the following.
- Pseudoesotropia. This is the appearance of an esotropia caused by the presence of a broad nasal bridge or prominent epicanthal folds and is more apparent when the infant is looking slightly off to the side.5
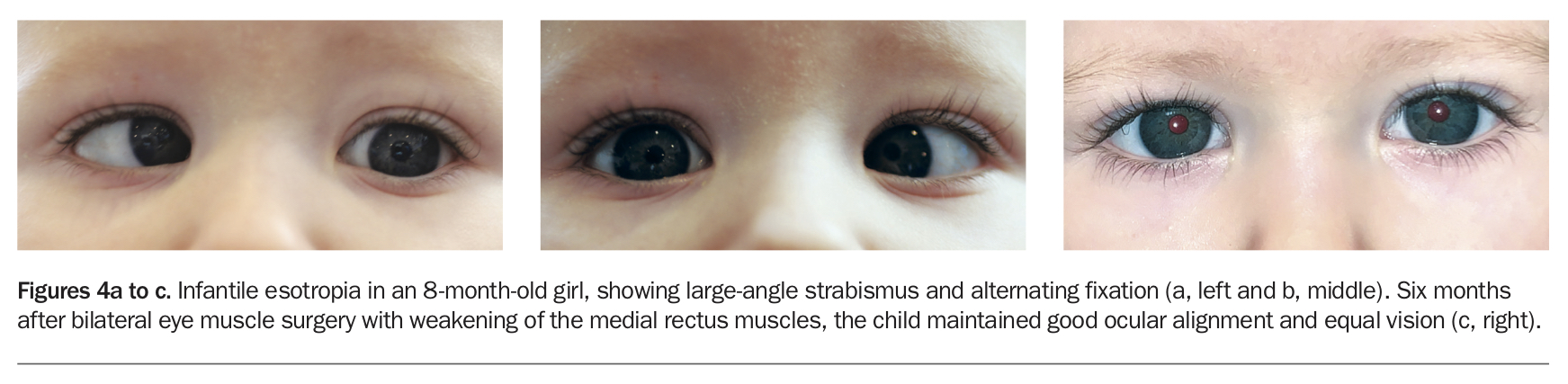
- Infantile esotropia. This is a constant, moderate-to-large-angle esotropia that presents after birth but before 6 months of age (Figure 4). Most children with infantile esotropia are in good general health and have no significant refractive error. Prompt referral is recommended, as surgical intervention before 12 months of age may allow the child to gain some binocular function.
- Accommodative esotropia. This usually presents in the second or third year of life and is associated with long-sighted refractive error. Initial treatment is full-time wearing of glasses. Any residual esotropia (despite the child wearing full-correction long-sighted glasses) requires eye muscle surgery.
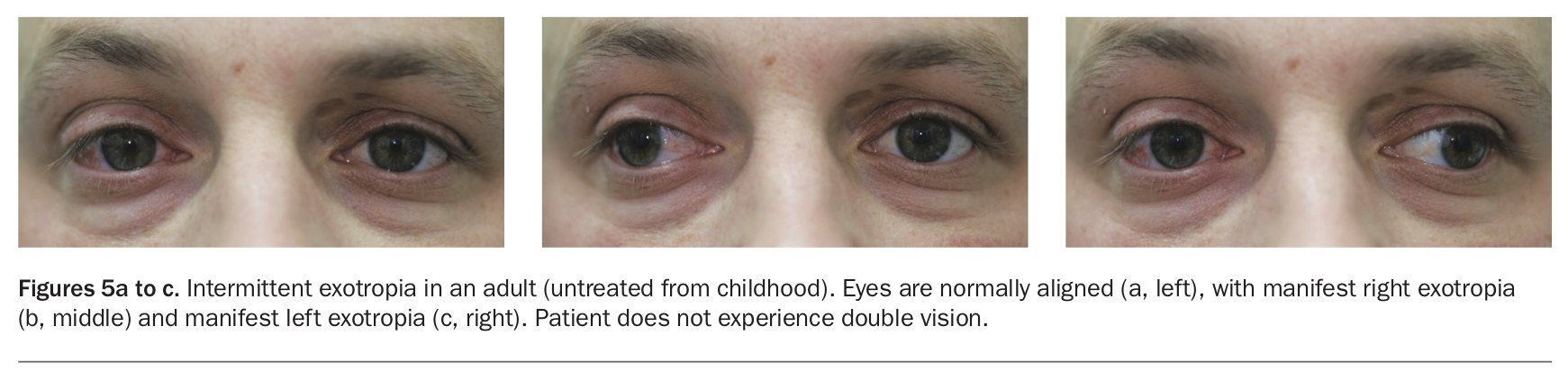
- Intermittent exotropia. This syndrome accounts for most exotropia in children and adults (Figure 5). It typically presents between 18 months and 5 years of age. The exotropia occurs intermittently under conditions of visual inattention, bright light or fatigue. It is most apparent when the child focuses far away in the distance. In most children with this condition, observation is sufficient management. Eye muscle surgery may be needed in a small proportion of patients.
{kind=link}
{kind=link}
A patient with new-onset double vision
The following cranial nerve palsies should always be considered in a patient of any age presenting with new-onset double vision. Temporal arteritis can cause cranial neuropathies in adults aged over 50 years.
- Oculomotor palsy. This must be considered in patients presenting with new exotropia. It is usually accompanied by a hypotropia, ptosis and, in some cases, dilation of the pupil. The pattern of clinical features is highly variable because most palsies are incomplete, and one or more extraocular muscles may be paretic. Urgent neuroimaging with cerebral angiography is recommended to exclude a life-threatening intracranial aneurysm, regardless of the pupil signs.
- Lateral rectus palsy. This can occur because of a microvascular insult, raised intracranial pressure or, rarely, after a viral illness. There is an esotropia for distance vision and a smaller or no esotropia for near vision. Abduction is limited on the affected side (Figure 2). An isolated microvascular palsy starts to recover within three months of onset. MRI of the brain is recommended to exclude an intracranial space-occupying lesion.
- Superior oblique palsy. This is the most common cause of vertical strabismus, with the affected eye being hypertropic (higher than the other). The patient usually adopts a head turn and head tilt away from the affected side. In contrast to oculomotor and lateral rectus palsies, there is no obvious limitation of eye movements. The most common cause of an acquired superior oblique palsy is closed head trauma. Bilateral asymmetrical involvement is common. Patients may report vertical or oblique double vision, along with some torsion (twisting). This is most noticeable during daily activities of walking downstairs or reading.
An adult with intermittent double vision
An adult presenting with intermittent double vision most likely has a decompensating latent or childhood strabismus. For example, decompensating exophoria is a latent strabismus that becomes intermittently manifest with ocular muscle fatigue (e.g. towards the end of the day, with alcohol intake or with concurrent systemic illness). Patients retain good binocular function most of the time but report double vision when the deviation is manifest.
In patients with intermittent symptoms, it is also important to consider the following.
- Myasthenia gravis. This presents with variable and fatiguable strabismus, often accompanied by ptosis. Any pattern of strabismus can occur. Half of all patients with myasthenia gravis present with isolated ocular involvement, and a further half of this group convert to generalised myasthenia in the course of their disease.6 Medical treatment is prescribed, and some patients may need eye muscle surgery.
- Cranial nerve palsy. Patients with lateral rectus palsy may only experience double vision for distance viewing and be asymptomatic when reading.
- Age-related distance esotropia. This is caused by involution of the orbital connective tissue pulleys, resulting in a small-angle esotropia for distance vision only. It is associated with other age-related periocular changes, such as involutional ptosis and limited upgaze. It must be differentiated from lateral rectus palsy through careful clinical examination.
A patient with thyroid disease and double vision
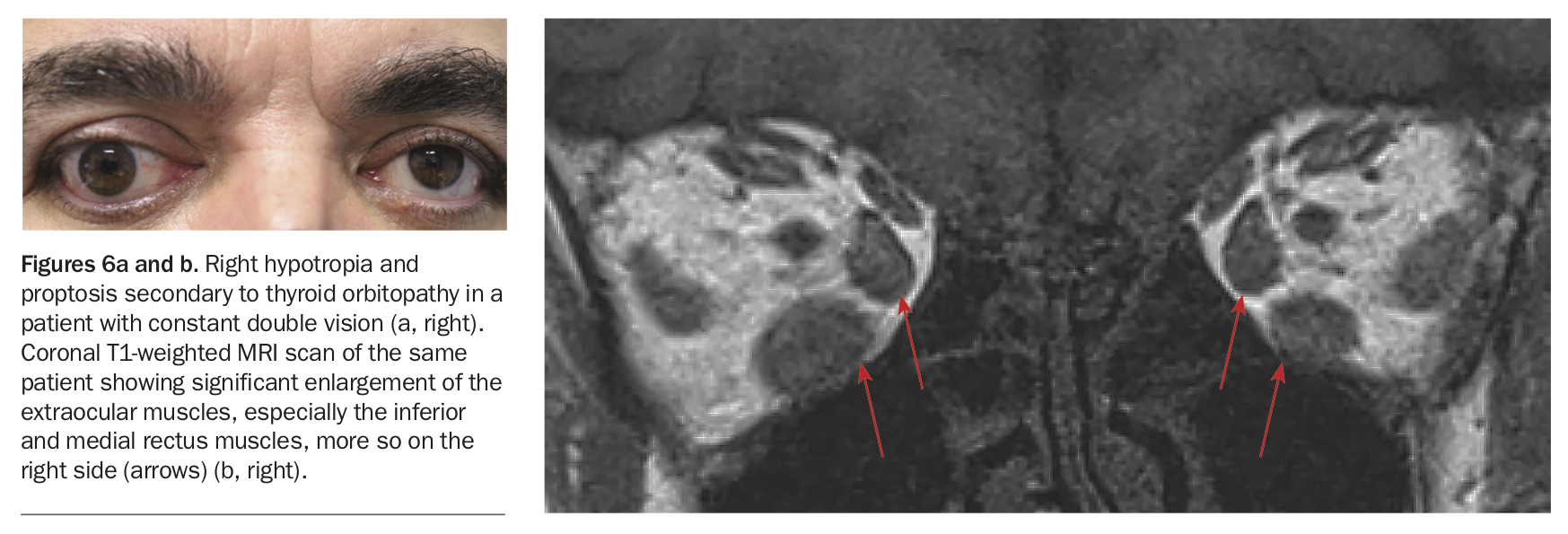
Thyroid orbitopathy is a complex disorder resulting from inflammation and infiltration of orbital tissues, including the extraocular muscles and orbital fat. It is usually associated with hyperthyroidism in Graves’ disease but can also occur in patients who are biochemically euthyroid or hypothyroid. There is proptosis (protrusion of the eyeball), exposure of the ocular surface and restrictive strabismus, with variable limitation of eye movements (Figure 6). The condition has a predilection for the inferior and medial rectus muscles, resulting in an esotropia, and asymmetrical involvement means that one eye is usually hypotropic compared with the other.
{kind=link}
Management is multidisciplinary and challenging. Active disease is controlled through thyroid suppression, systemic immunosuppression and/or orbital radiotherapy. Vision-threatening disease with corneal exposure or optic nerve compression from enlarged extraocular muscles requires intravenous methylprednisolone and possibly urgent orbital decompression. Double vision during this phase is managed with occlusion of one eye. When the disease has stabilised, attention is directed towards managing proptosis, strabismus and eyelid position. Orbital decompression is performed for proptosis if needed, followed by eye muscle surgery. The result of surgery in thyroid orbitopathy is highly unpredictable because of altered muscle contractility and fibrosis, so a staged approach is generally recommended to avoid overcorrection.
A patient with a longstanding strabismus and abnormal appearance
Many children and adults live with strabismus as part of their identity. These patients may benefit from reconstructive eye muscle surgery to restore normal appearance and improve their psychosocial function and quality of life. This surgery is not considered to be cosmetic. Improved eye alignment through eye muscle surgery can reduce alienation and bullying for school-aged children.7 In adults, eye muscle surgery can improve social interactions and employability.8
Conclusion
Strabismus is a common condition in children and adults, with significant functional and psychosocial impact. There are a few conditions accounting for most cases of strabismus seen in general practice. Management options will depend on the underlying cause, and most patients with strabismus should be referred to an ophthalmologist for management. Eye muscle surgery is highly successful and often the best treatment option. MT
Further reading
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.