Immunotherapy for cancer and immune-related adverse events
Immune checkpoint inhibitors that remove the ‘brakes’ on the body’s immune system, enhancing its attack on cancer cells, have revolutionised the treatment of many cancers. However, these medications can cause a wide range of immune-related adverse events that GPs need to be aware of.
Immunotherapy with checkpoint inhibitors has revolutionised the treatment of many cancers. These medications have provided durable responses and excellent long-term outcomes in a substantial subset of patients with a range of cancer types, including melanoma, renal cell carcinoma and non-small cell lung cancer.1 Immune checkpoints are regulators that modulate physiological immune responses and maintain self-tolerance.2 Checkpoint inhibitors can disrupt this interaction and enhance the activity of the immune system against cancer cells. However, they can also induce inflammatory and other immune-related adverse events (AEs).3
With the increasing use of checkpoint inhibitors and improving patient survival, GPs will have growing numbers of patients receiving these medications and need to be aware of the potential AEs. In this article, we review the checkpoint inhibitors currently in use in Australia and the possible immune-related AEs they can induce. We aim to increase awareness of these AEs and how to approach management of patients receiving checkpoint inhibitors in general practice.
What is immunotherapy?
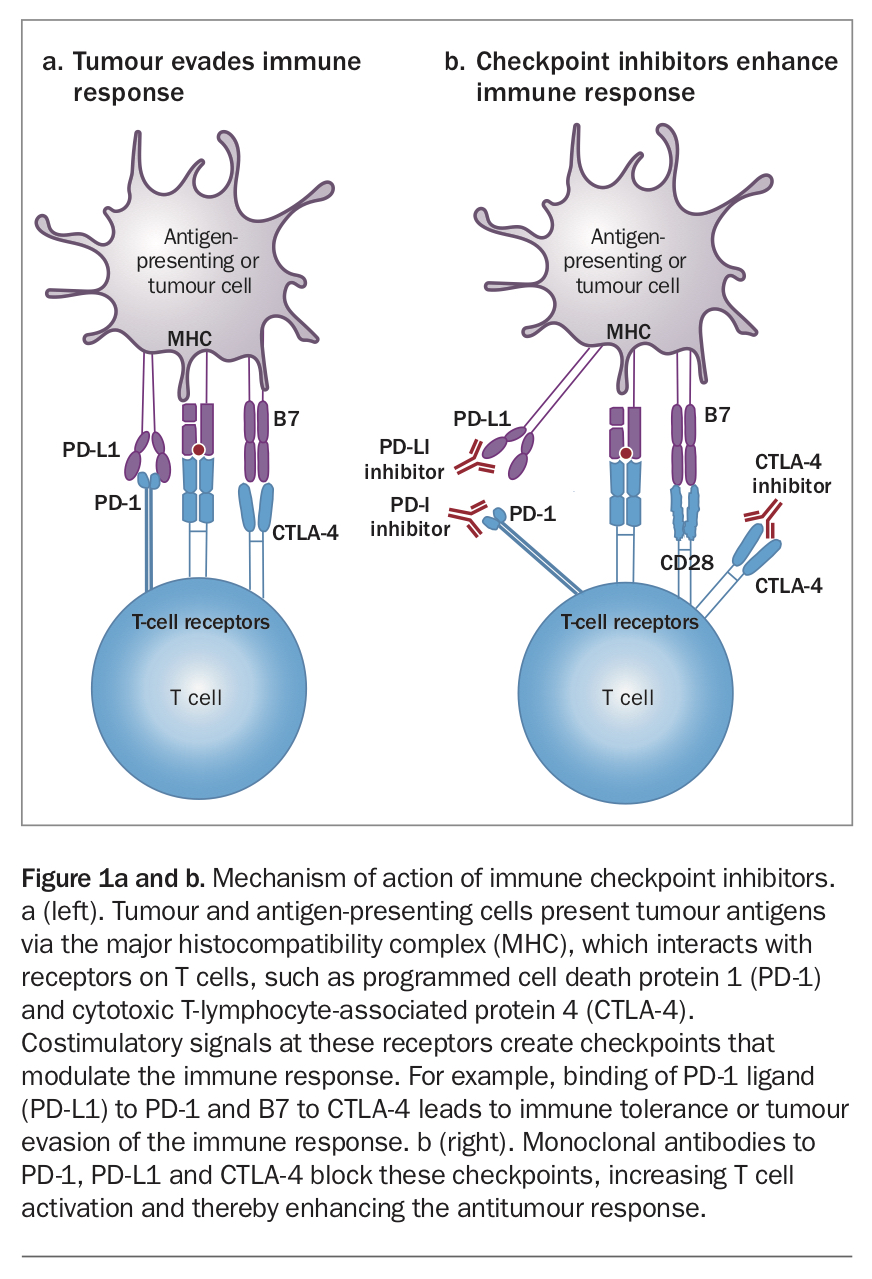
Self-tolerance, or the ability of the immune system to recognise and avoid attacking self, is maintained via a plethora of checkpoints within the immune cascade that modulate immune responses.4 Tumour cells can ‘take advantage’ of these normal immune checkpoints to reduce the effectiveness of antitumour immunity (Figure 1a).1-3 Molecules involved in these checkpoint pathways include T-cell receptors such as programmed cell death protein 1 (PD-1) and cytotoxic T-lymphocyte-associated protein 4 (CTLA-4), and the PD-1 ligand (PD-L1).
{kind=link}
Blocking the immune checkpoints with monoclonal antibodies (checkpoint inhibitors) can release the so-called ‘brakes’ on the immune system, potentially enhancing antitumour immunity (Figure 1b). Monoclonal antibodies to PD-1, PD-L1 and CTLA-4 have been shown to produce durable antitumour responses.1,2,5
Immunotherapy with checkpoint inhibitors differs from traditional cancer therapy with cytotoxic agents that target the cell cycle. The latter lead to numerous side effects, including alopecia, bone marrow suppression (with possible febrile neutropenia), nausea and vomiting, peripheral neuropathies and infertility.6 In contrast, immunotherapy can result in inflammatory and other immune-related AEs that have not traditionally been seen with cytotoxic therapies.
What are the indications for immunotherapy?
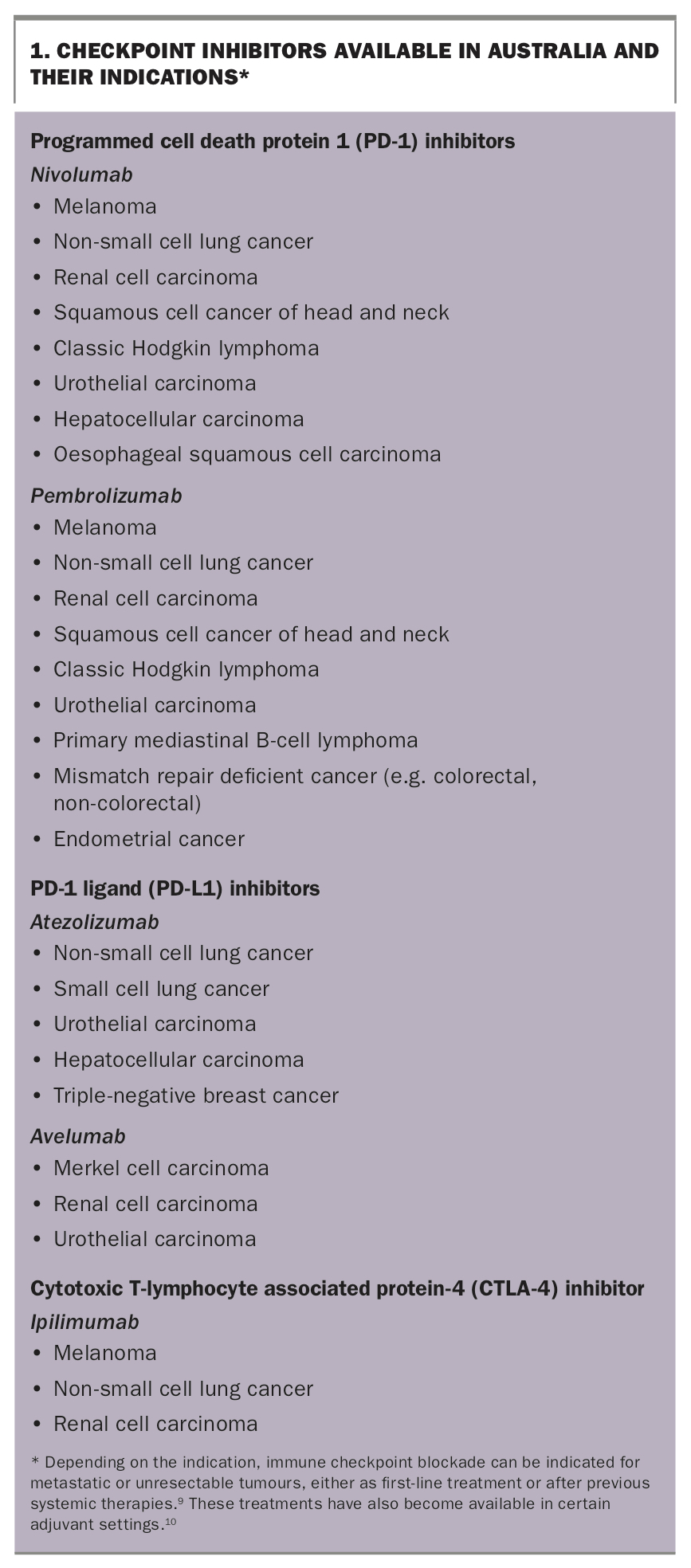
The indications for checkpoint inhibitors are expanding across malignancies.7 Checkpoint inhibitors registered for use in Australia comprise:
- two PD-1 inhibitors (nivolumab and pembrolizumab)
- two PD-L1 inhibitors (atezolizumab and avelumab)
- a CTLA-4 inhibitor (ipilimumab).8
The indications for these medications are listed in Box 1.9,10 Many more checkpoint inhibitors are available via expanded access programs and are being investigated in clinical trials.
{kind=link}
Why do immune-related adverse events occur?
The therapeutic benefits of checkpoint inhibitors can be complicated by immune-related AEs caused by the unleashing of the brakes on immune tolerance. As well as increasing immune system activity directed against tumour cells, this can lead to autoimmunity. It is plausible for any autoimmune or autoinflammatory manifestation to occur as an AE, although the nature and treatment can differ from ‘classic’ autoimmune diseases.
What are the potential adverse events?
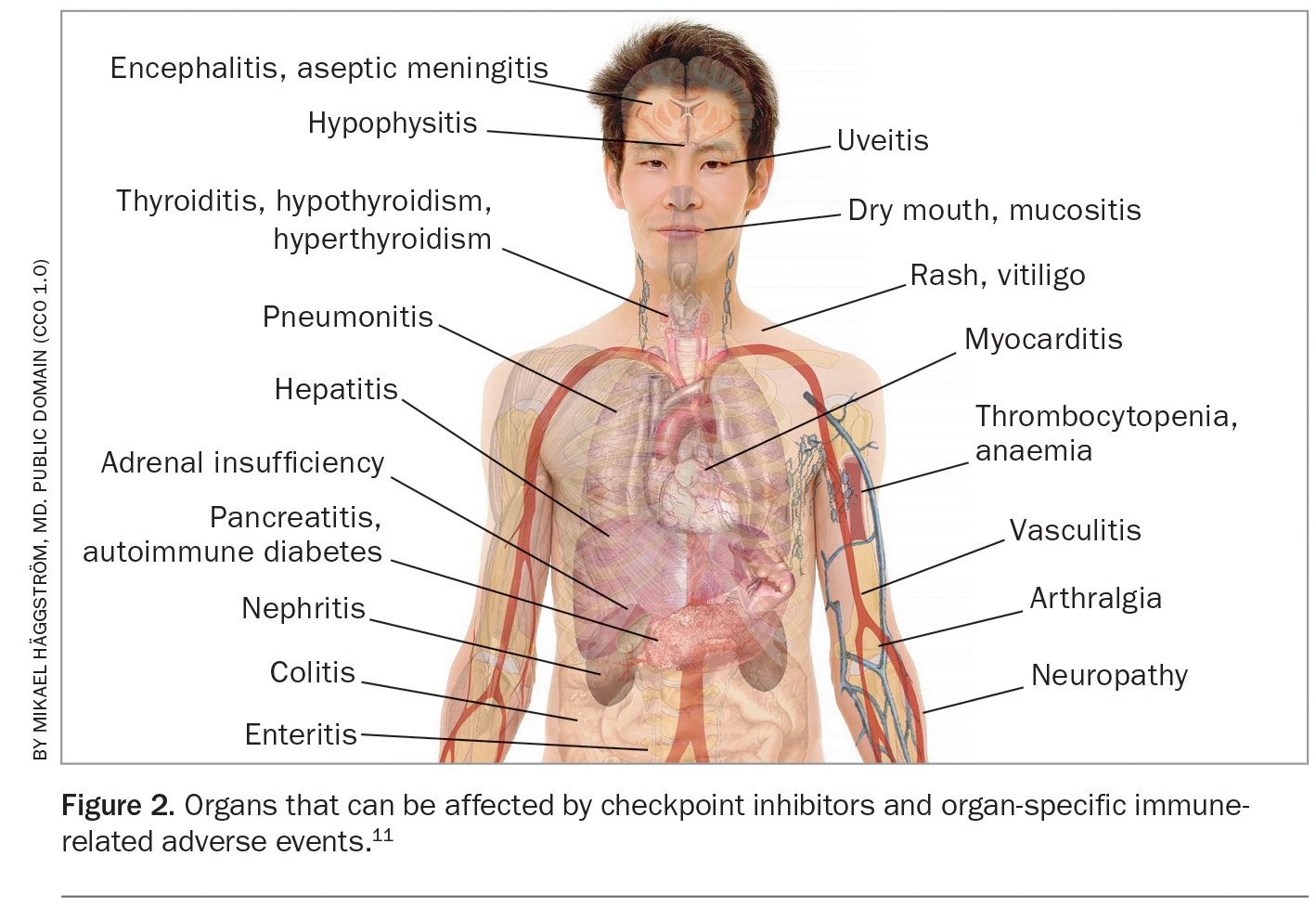
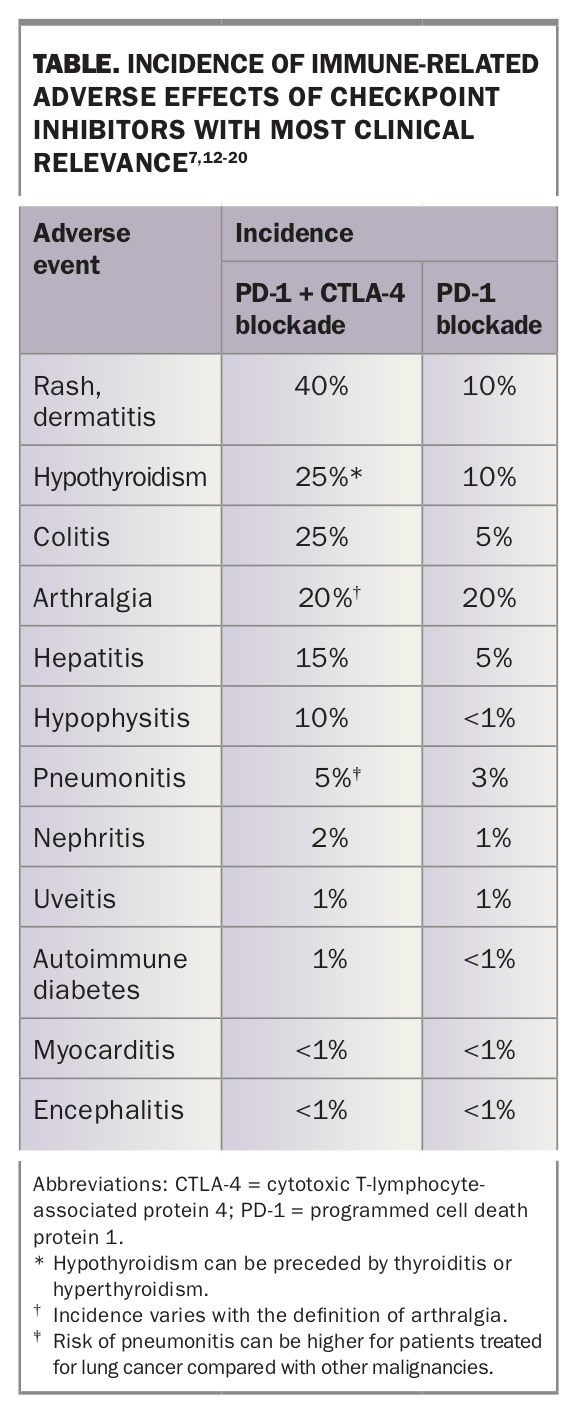
The spectrum of immune-related AEs is wide. Symptoms can range from mild, where immunotherapy can be continued or resumed after a brief interruption, to severe or even life-threatening, necessitating permanent discontinuation of immunotherapy.11 Although any tissue or organ can be involved, immune-related AEs most commonly affect the skin, colon, endocrine organs, liver and lungs.3,11 Cardiac and neurological immune-related AEs are less common but can be dangerous and even life-threatening.3 The organs that can be affected by checkpoint inhibitors and organ-specific immune-related AEs are shown in Figure 2 and the Table.7,11-20
{kind=link}
{kind=link}
This wide array of AEs can be graded for severity on a scale of 1 to 5 using the Common Terminology Criteria for Adverse Events (CTCAE).21 This classification system is used by oncologists for clinical trials; management also often depends on the severity or grade of the AE.
Immune-related AEs can occur at any time, even months after discontinuing treatment. However, the median onset is within two to 16 weeks of commencement of therapy.22
Can we predict adverse events?
Studies have indicated that a history of autoimmune disease and the use of combination immunotherapy with both PD-1 or PD-L1 plus CTLA-4 inhibitors increase the risk for developing immune-related AEs.22 Patients with pre-existing autoimmune disease have been excluded from clinical trials. However, retrospective data have been encouraging for the use of checkpoint inhibitors in these patients.23 Other likely factors include genetics, previous infections and treatments, the microbiome and environmental factors.24
Ultimately, the balance between the cancer versus the risk of an immune-related AE needs to be discussed between the patient and doctor.25 The incidence of severe (grade 3 to 4) AEs is about 20 to 25% for anti-PD-1 therapy alone, and about 55 to 60% for combination immunotherapy.26
What are the organ-specific adverse events?
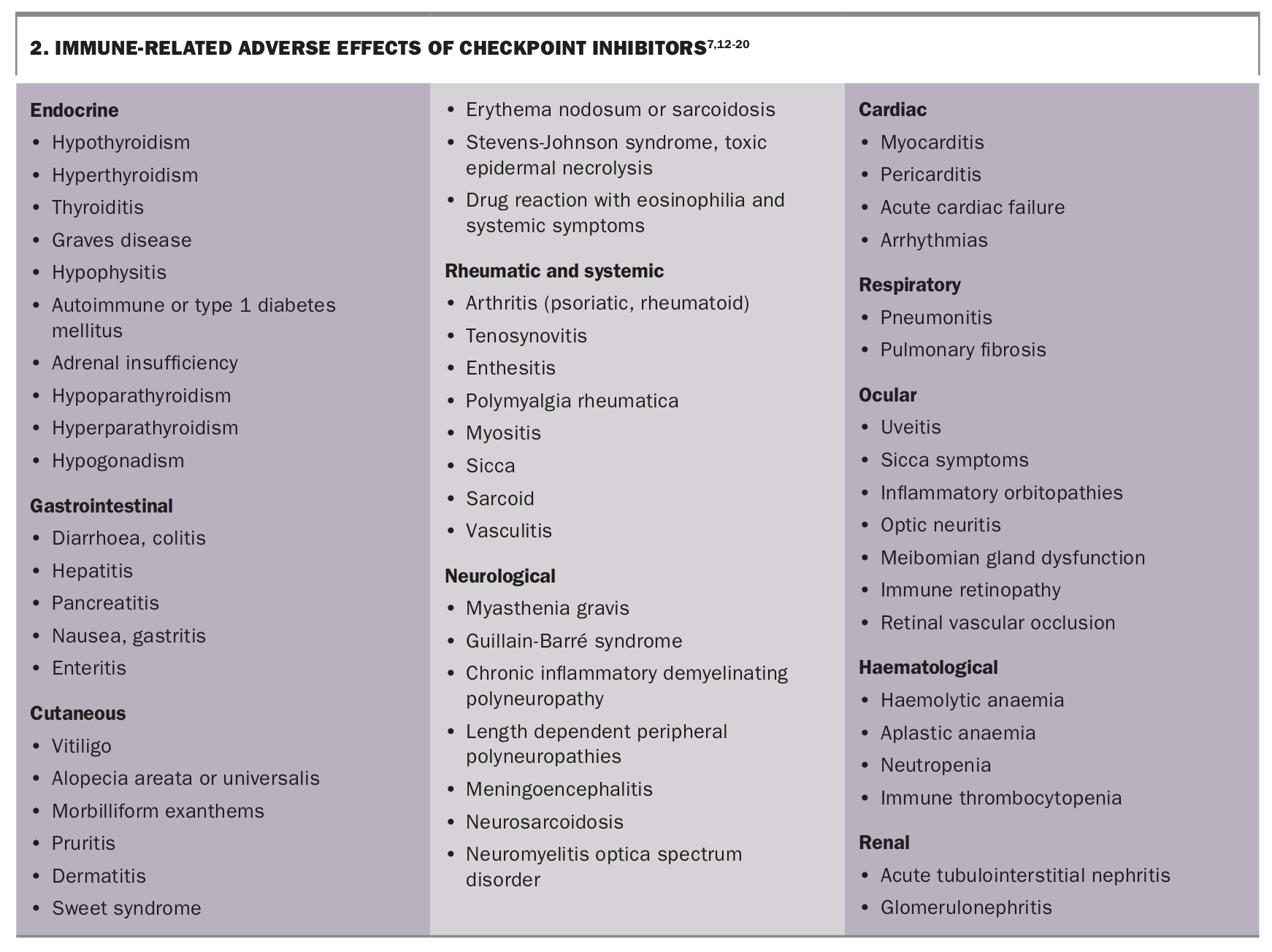
The immune-related AEs of greatest clinical importance and their incidence are listed in the Table.7,12-20 A more extensive list of organ-specific manifestations appears in Box 2.7,12-20 Further information and guidance can be obtained from the European Society for Medical Oncology and American Society of Clinical Oncology guidelines.3,27
{kind=link}
How are patients with AEs treated?
Treatment depends on which organ system is affected and the severity (grade) of the toxicity based on the CTCAE classification.3,21 Many therapeutic algorithms have been suggested to assist in the diagnosis and management of immune- related AEs.
- Patients with mild immune-related AEs (grade 1) do not always require therapy and can often be carefully monitored and continue on the checkpoint inhibitor.
- If immune-related AEs become more severe, treatment discontinuation is essential, and immunosuppressive agents are frequently required alongside referral to the relevant specialist.
- In severe cases, checkpoint inhibitor therapy needs to be discontinued permanently.
- Glucocorticoids are the mainstay of therapy, except for patients with endocrine immune-related AEs, where hormone replacement is usually sufficient. Hormone replacement may be required lifelong as recovery from immunotherapy-induced endocrinopathies is rare.
What is the GP's role?
In this era of increasing use of immunotherapy, GPs will encounter immune-related adverse events more frequently. Immune-related AEs can present in unusual and unpredictable ways, different from classic autoimmune or autoinflammatory diseases. In rare cases, they can be life-threatening (e.g. neurotoxicity and cardiomyopathy) or permanent (e.g. diabetes mellitus). Although therapeutic algorithms exist, treating immune-related AEs is challenging and requires a highly individualised approach that needs to be initiated and coordinated by an experienced oncology team.
A high index of clinical suspicion and early recognition of immune-related AEs are essential. If an immune-related AE is suspected in general practice, prompt communication with the treating oncology team is essential to initiate diagnostic work-up and further management. Clinical practice points on immunotherapy and immune-related AEs are summarised in Box 3.
Conclusion
Immunotherapy with checkpoint inhibitors has improved the responses to malignancies that have traditionally had poor outcomes. As use of these therapies is expanded, we will increasingly encounter side effects such as immune-related AEs that differ to those seen with traditional cytotoxic agents. The detection and management of these clinically heterogeneous immune-related AEs is complex and requires multidisciplinary input and co-ordination by the oncology team. Early recognition of immune-related AEs is crucial and depends on a high index of clinical suspicion. If an immune-related AE is suspected in general practice, prompt communication with the treating oncology team is essential. MT
COMPETING INTERESTS: Dr Dey is an Advisor for Janssen and has received educational sponsorship from Pfizer and Janssen. Professor Long has been a Consultant Advisor for Aduro Biotech, Amgen, Array Biopharma, Boehringer Ingelheim International, Bristol-Myers Squibb, Highlight Therapeutics, Merck Sharpe and Dohme, Novartis Pharma, Pierre Fabre, QBiotics Group and Regeneron Pharmaceuticals. Associate Professor Schrieber is a Consultant Advisor for Pfizer Australia and Boehringer Ingelheim. Dr Rogiers: None.
ACKNOWLEDGEMENTS: Dr Rogiers is supported by a Cameron Fellowship at Melanoma Institute Australia.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.