A Cervical Screening Program update: the intermediate risk pathway, the co-test and self-collection

Cervical screening guidelines have changed significantly in recent years and continue to evolve as evidence about human papillomavirus testing emerges, especially regarding intermediate risk results and the role of self-collection.
The renewed National Cervical Screening Program (NCSP) was implemented in November 2017 following extensive modelling studies, which showed that a switch from cytology testing to primary human papilloma virus (HPV) testing in the context of the school-based HPV vaccination program would result in up to 30% fewer cancers.1 In the renewed NCSP, screening occurs every five years from the age of 25 until a final exit test between 70 and 74 years of age. The Cancer Council Australia Guidelines provide comprehensive clinical practice guidance for primary care and specialist clinicians and is updated to reflect emerging evidence.2 The introduction of the NCSP was also accompanied by a change from state- and territory-based registries to a single National Cancer Screening Register (NCSR), responsible for all screening invitations and reminders for eligible people. The NCSR Healthcare Provider Portal is now accessible via a PRODA account through most medical record software programs, enabling point of care access to a patient’s screening history, which can be updated by healthcare providers as well as laboratories and patients.
In this article, we provide updates on a recent change to the intermediate risk pathway and review the role of the co-test both for patients with symptoms and patients who require a ‘Test of Cure’ (ToC) after treatment for a histologically proven high-grade lesion. We also consider the current and future role of screening with self-collection of a vaginal sample in relation to new evidence of its comparable effectiveness to clinician-collected samples, published since the implementation of the renewed NCSP.
In this article, although we refer to ‘women’, we acknowledge that the information is relevant for anyone with a cervix, including transgender and gender diverse people.
Updated intermediate risk pathway
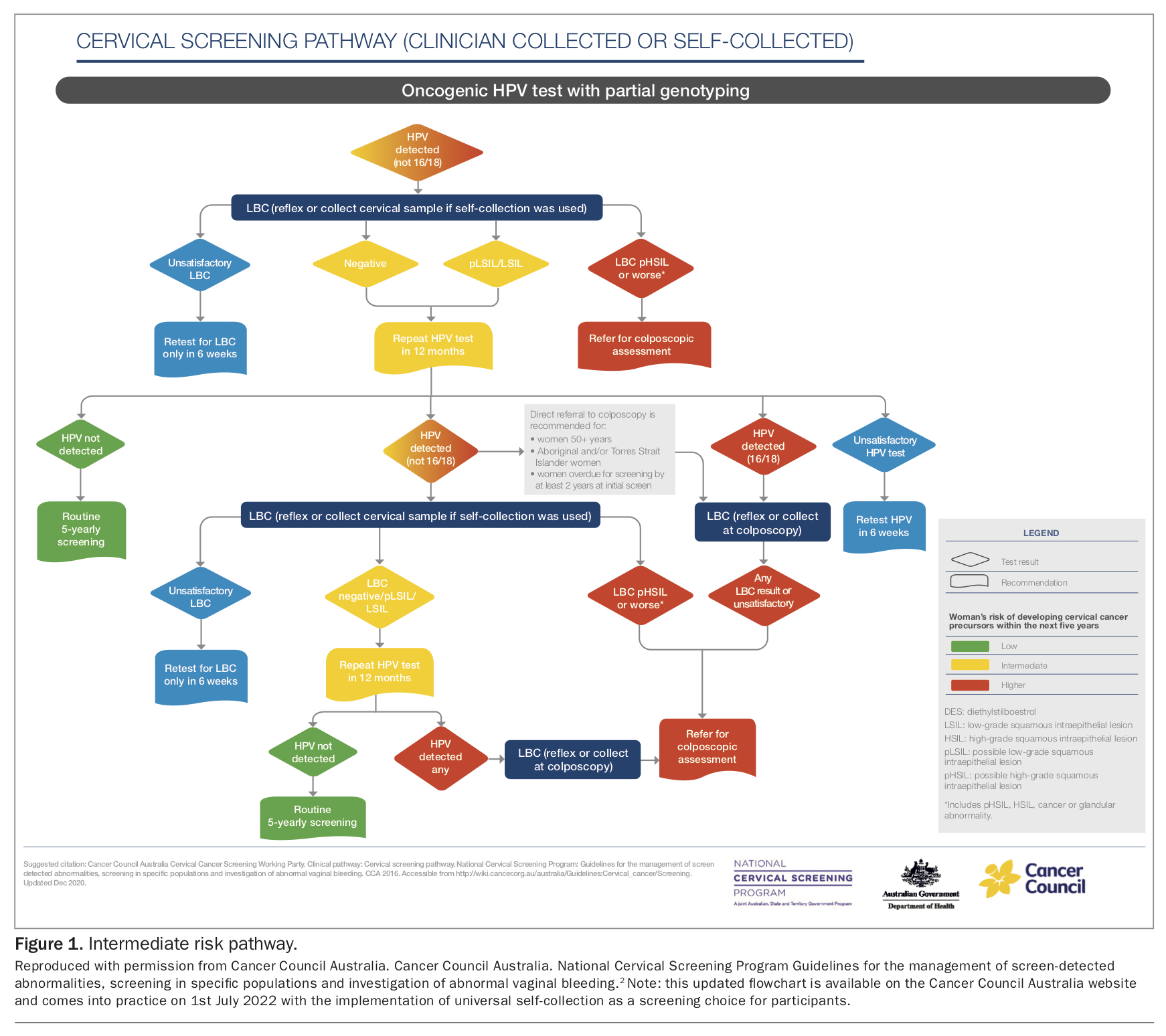
The Cervical Screening Test (CST) tests for 14 oncogenic HPV types known to be associated with cervical cancer, with reflex liquid-based cytology (LBC) performed automatically by the laboratory if the test is positive for any oncogenic HPV type. The results are stratified by risk into low, intermediate and higher risk categories. An intermediate risk result is one in which one or more of the 12 HPV (not 16 or 18) types is detected and LBC is either negative or predictive of possible or actual low grade intraepithelial neoplasia (pLSIL/LSIL).
When the NSCP was first implemented, a cautious approach to intermediate risk screening results was adopted. The recommendation was for a follow-up HPV test 12 months later and if HPV (any type) was detected, referral for colposcopy was advised regardless of the reflex LBC result. However, an analysis of colposcopy and biopsy outcomes for the first two years of the renewed NCSP among this group confirmed the impressions of colposcopists that the risk of cervical intraepithelial neoplasia (CIN) 2 or worse was very low compared with other groups referred for colposcopy. After expert review of this emergent evidence, a change to the guidelines was instigated.3
Since 1st February 2021, most patients in whom HPV (not 16 or 18) is again detected at the 12-month HPV follow-up test can be safely advised to have a second HPV test in another 12 months, as long as their reflex LBC was reported as negative or pLSIL/LSIL. If HPV (not 16 or 18) infection still persists at this time (24 months after the initial intermediate risk CST result), referral for colposcopy is recommended regardless of the cytology result (Figure 1). Given that most HPV infections will clear without medical intervention in 12 to 24 months, these new recommendations are expected to avoid many unnecessary colposcopies and associated harms, including the possibility of biopsy and overtreatment as well as anxiety and financial costs.4 Given the extensive waiting lists for colposcopy in some services, this change will also divert services towards those patients with a higher likelihood of biopsy-proven high grade pre-cancerous lesions that will require treatment.
{kind=link}
Good communication is essential for allaying anxiety around abnormal cervical screening results. An intermediate risk cervical screening test result could be explained to a patient as follows:
‘Your test shows that you do not have one of the main cancer-causing HPV types (16 or 18), but the test found one of the other HPV types, which could rarely lead to cancer in many years from now. In almost all cases, the body’s immune system clears the virus within one to two years but often within a year, and to check if this has happened, we will follow up in 12 months from now with another test.’
Exceptions to the updated intermediate risk pathway
Although this updated pathway for persistent HPV (not 16 or 18) after an intermediate risk CST result applies to most patients, exceptions are in place for individuals who may be at higher risk of an underlying high-grade abnormality even in the presence of a negative or low-grade cytology result (Figure 1). This includes patients who are:
- aged 50 years or older
- Aboriginal and/or Torres Strait Islander
- two or more years overdue for their initial CST.
Patients in these groups should be referred for colposcopy if HPV (not 16 or 18) is again detected at the 12-month follow-up test, regardless of the LBC result. Pathology laboratories play an essential role in providing management recommendations to the referring clinician. It is important for the clinician to add Aboriginal and/or Torres Strait Islander identification information to the pathology request form, as this will assist the laboratory to identify that the patient is at higher risk of an underlying high grade abnormality at the 12-month follow-up test if HPV (not 16 or 18) is detected again, and prompt inclusion of a recommendation for referral to colposcopy in the laboratory report.
The role of the co-test in the NCSP
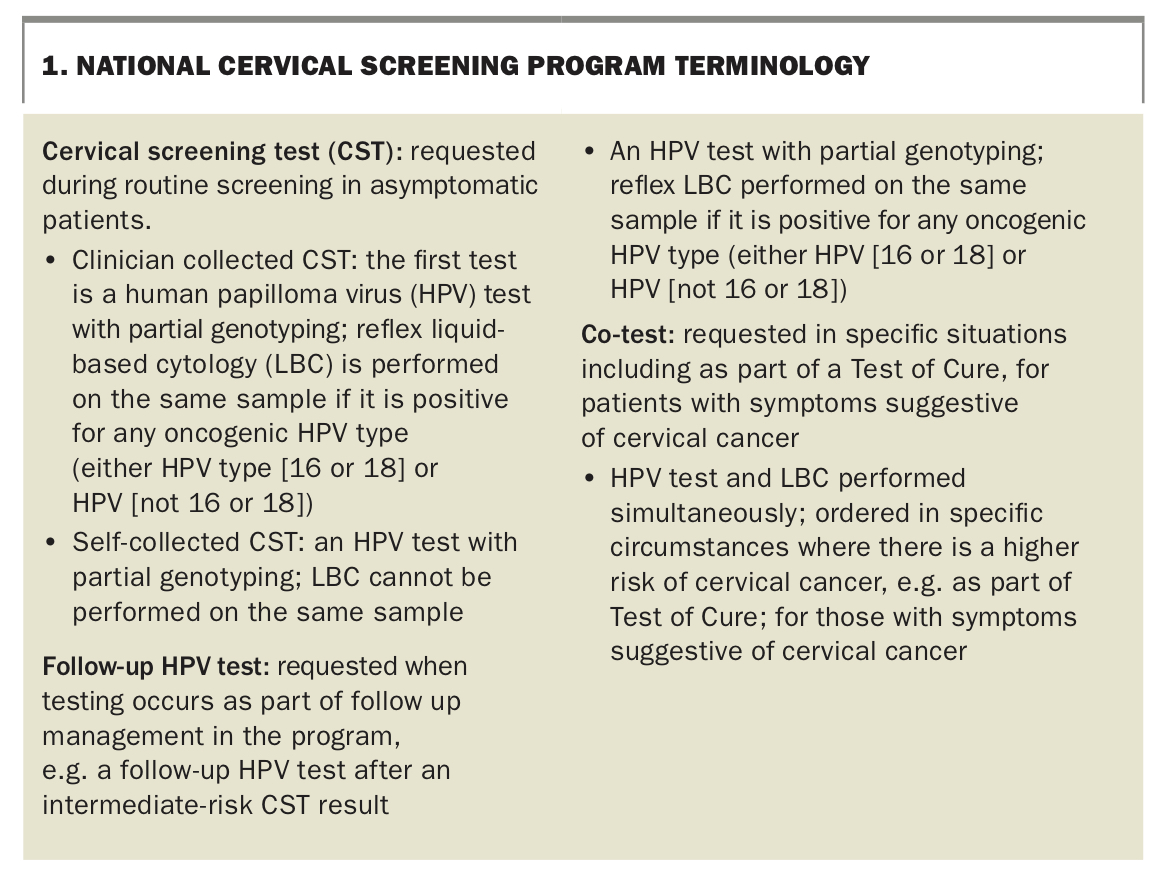
The co-test is an HPV test and LBC performed simultaneously by the laboratory, with both results provided to guide clinical management. It is not a screening test, but rather a test used to investigate patients considered to be at higher risk of malignancy because it has slightly increased sensitivity compared with an HPV test in the presence of blood, as well as a high negative predicitive value in detecting those at risk of disease recurrence following treatment. NCSP terminology is explained in Box 1.
{kind=link}
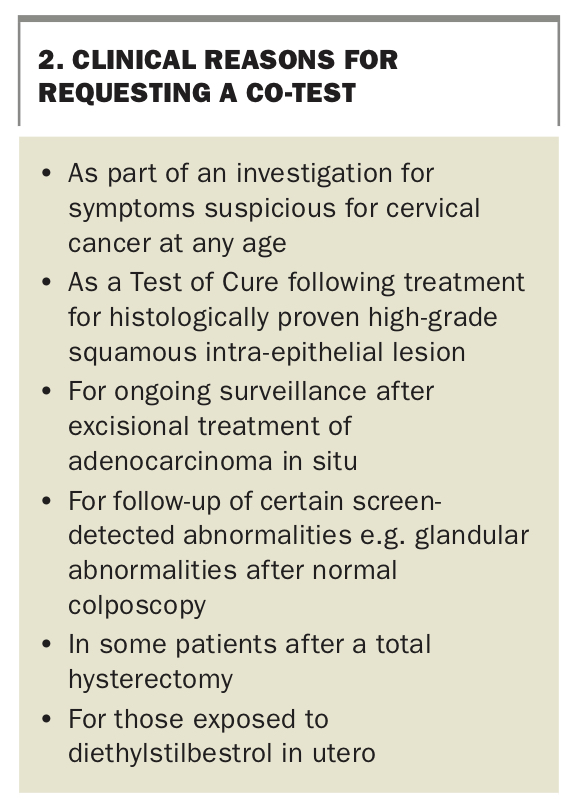
It is essential to add the reason for the co-test on the pathology request form in order to inform an appropriate management recommendation from the laboratory. Box 2 shows the specific situations when a co-test should be requested. Given that a positive co-test is associated with a lower threshold for colposcopy referral than a CST, it is important to be aware that inappropriate use of a co-test can lead to unnecessary colposcopy referrals and potentially to unnecessary biopsies and overtreatment. Early findings in the renewed NCSP suggested that application of the co-test for symptoms may have differed between clinicians, with anecdotal reports of overuse.5 This led to further clarity in the definition of the relevant signs and symptoms that warrant a co-test.
{kind=link}
The co-test for symptoms suspicious for cervical cancer
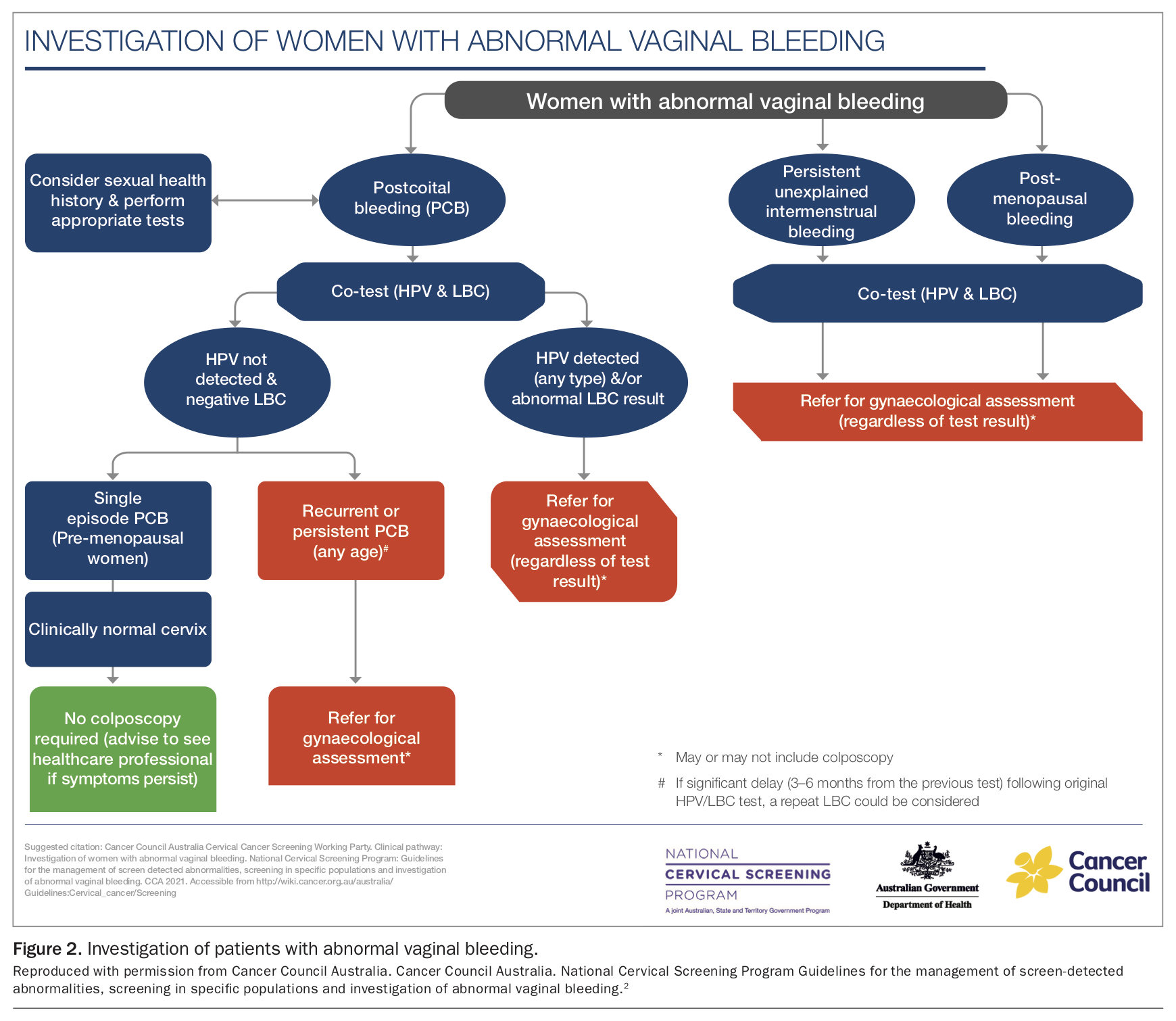
The co-test is an important tool for investigating patients with symptoms suspicious for cervical cancer and should not be delayed by the presence of blood (Figure 2). However, it is important to remember that in the vast majority of patients, abnormal bleeding, especially in younger patients, will relate to a benign cause and not cervical cancer. Common causes of abnormal vaginal bleeding that need to be considered include sexually transmitted infections (STIs), particularly chlamydia, hormonal contraceptive-related bleeding and cervical polyps.
{kind=link}
Co-testing or a colposcopy referral are not required in the following situations, although a CST would be taken if due:
- breakthrough bleeding or irregular bleeding due to hormonal contraception
- heavy regular bleeding (heavy menstrual bleeding)
- irregular bleeding, including postcoital bleeding (PCB) in the setting of an STI that stops after treatment
- contact bleeding with routine CST and no other symptoms.
If a co-test is warranted on the basis of the patient’s history, it is essential to document the reason for requesting a co-test on the pathology request form in order to inform laboratory recommendations.
Postcoital bleeding - a red flag for cervical disease
Postcoital bleeding (PCB) is a red flag sign for cervical disease, especially when unexplained, persistent or recurrent.6 Although most cases of PCB are associated with benign causes, such as chlamydia infection or a cervical polyp, a co-test should be considered for patients of any age presenting with this symptom. If there has been a single episode of PCB and any component of the co-test is positive, including a low-grade cytology result, colposcopy referral is recommended. However, if the co-test is negative for both HPV and LBC and clinical examination of the cervix is normal, colposcopy referral is not required for a single episode of PCB. In these cases, it is essential to ensure the patient knows to return for review if PCB recurs or persists as this requires referral for colposcopy, regardless of a normal clinical examination and a negative co-test.
Intermenstrual and post-menopausal bleeding
Patients of any age with intermenstrual bleeding should be assessed for common causes such as STIs or bleeding associated with hormonal contraception. Investigation with a co-test and referral to a gynaecologist is recommended for patients with intermenstrual bleeding that remains unexplained because of the possibility of cervical disease. Patients with post-menopausal bleeding are also recommended to have a co-test as part of an investigational work-up and should be referred to a gynaecologist regardless of the result.
Unexplained persistent vaginal discharge or deep dyspareunia
Unexplained persistent and unusual vaginal discharge, especially if it is offensive and blood stained, can be a rare presentation of advanced cervical cancer and warrants a co-test and referral. By contrast, unexplained persistent deep dyspareunia is very unlikely to be associated with cervical cancer; therefore, a CST (if due) rather than a co-test, as well as referral for gynaecological assessment, are recommended.6
The co-test as 'Test of Cure'
The co-test is used during the ToC pathway after treatment of a histologically-proven high-grade abnormality as its high negative predictive value confirms both treatment success and absence of early recurrence. The co-test is performed 12 months after treatment and annually thereafter until both the HPV and LBC components are negative on two consecutive occasions, after which the patient can return to five-yearly routine screening. Colposcopy referral is required if HPV 16 and/or 18 is detected at any time during ToC, regardless of the LBC result, as well as if the LBC is predictive of a possible or actual high-grade abnormality, regardless of HPV status. If HPV (not 16 or 18) is detected and/or the LBC is predictive of a possible or actual low-grade abnormality at any time during ToC an annual co-test is performed until both components are negative on two consecutive occasions. If these results continue to fluctuate specialist discussion and referral can be considered.
Based on available evidence, patients diagnosed with adenocarcinoma in situ (AIS) are recommended to have annual co-tests for life.
The co-test is also performed in some situations for those who have undergone a total hysterectomy with removal of the cervix, and a systematic approach is needed to determine whether follow-up with a vaginal vault test is required. The patient’s cervical screening history, the reason for the hysterectomy (benign or malignant disease) and histopathology results for any cervical tissue are important factors that influence the management pathway.7 Women with a total hysterectomy for benign disease do not require ongoing surveillance if both of the following apply, as their risk of vaginal cancer is no higher than for the general population:
- a negative screening history or treated for a histologically confirmed high-grade abnormality with completed ToC
- no evidence of cervical pathology on the hysterectomy specimen.
For those at higher risk of cervical cancer, a vaginal vault co-test is taken at 12 months post-total hysterectomy and then annually until two negative consecutive co-tests, with colposcopy referral recommended for any positive oncogenic HPV type and/or cytological abnormality. The vaginal co-test is taken with a sampler (Figure 3), which is swept circumferentially around the proximal blind end of the vault. Patients who have had a hysterectomy and been treated for cervical or endometrial cancer have an increased risk of recurrent vaginal vault cancer and require ongoing surveillance by a gynaecological oncologist.
{kind=link}
Exposure to diethylstilbestrol in utero
Diethylstilbestrol (DES) was used for a number of pregnancy-related problems including threatened miscarriage in the 1940s until its use was banned in the early 1970s. Exposure to DES in utero is associated with a higher risk of rare clear cell adenocarcinoma of the vagina and cervix, which occurs in about one per 1000 of those exposed. These women should be offered annual co-test and specialised colposcopic examination of both the cervix and vagina indefinitely.
Self-collection within the NCSP
The change from cytology-based screening to HPV-based screening in 2017 presented the opportunity to include self-collection of a vaginal swab within the program. Its inclusion recognised the importance of removing barriers to screening for under- and neverscreened people, who account for more than 70% of those diagnosed with cervical cancer.8 Recent evidence has found that self-collection is an acceptable option amongst underscreened populations.9 Although data are limited, the following groups are more likely to be under- or never-screened:
- Aboriginal and Torres Strait Islander people
- people living in rural and remote areas
- people living in low socioeconomic areas
- those of culturally and linguistically diverse (CALD) backgrounds
- individuals with a history of sexual violence and trauma
- people who identify as lesbian, gay, bisexual, transgender, intersex or questioning, including transgender men with a cervix.
A cautious approach to self collection was initially taken, with eligibility for access to self-collected vaginal HPV tests restricted up to 1st July 2022 to individuals aged 30 years and above who are at least two years overdue for a CST or never screened who decline a speculum examination. Uptake of the self-collection pathway has been significantly lower than predicted based on the number of potentially eligible participants, which is likely due to a combination of provider awareness and confidence in this approach, difficulty in determining whether a patient meets the eligibility criteria, lack of awareness of this option by participants and the limited number of laboratories accredited to perform HPV testing on self-collected samples.10
Soon after the implementation of the renewed NCSP, a 2018 updated meta-analysis showed that the sensitivity and specificity of HPV testing to detect CIN 2 and higher in self-collected samples were similar to those for clinician collected samples when using validated PCR tests.11 Based on this and other evidence, a review by the Medical Services Advisory Committee (MSAC) in March 2021 concluded that HPV testing using self-collected samples is just as accurate as clinician-collected samples and that making self-collection available to more people is expected to better achieve the aim of increasing participation rates in the cervical screening program.12 In November 2021, the Minister for Health approved universal self-collection as a choice for anyone eligible for routine screening within the NCSP from 1st July 2022. This promises to be a ground-breaking strategy for overcoming barriers to screening, including shame, stigma and fear associated with a speculum examination.
Self-collection is offered under the supervision of a healthcare professional and involves the provision of information about the test and what is recommended in the event that oncogenic HPV is detected. Patients should be aware that LBC cannot be performed on a self-collected sample. Most people having a self-collected test will be negative for HPV and can be reassured that the risk of cervical cancer is very low and invited to re-screen in five years. However, around 2% of those attending for routine screening (varying with age) will be expected to have HPV 16 and/or 18 detected and will be referred directly for colposcopy, whereas around 6% will be expected to have HPV (not 16 or 18) detected. This group will be advised to return for a clinician-collected LBC to inform the recommendation of either immediate colposcopy referral or a follow up HPV test in another 12 months.13 Patients requiring a co-test, including those with symptoms, patients who are undergoing ToC after treatment of a high-grade lesion or patients exposed to DES in utero, are not eligible for a self-collected sample. The updated self-collection pathways are now available on the Cancer Council Australia website and will be fully incorporated into the National Cervical Screening Guidelines on 1st July 2022, when the universal choice of self-collected cervical sampling is made available through the NCSP.
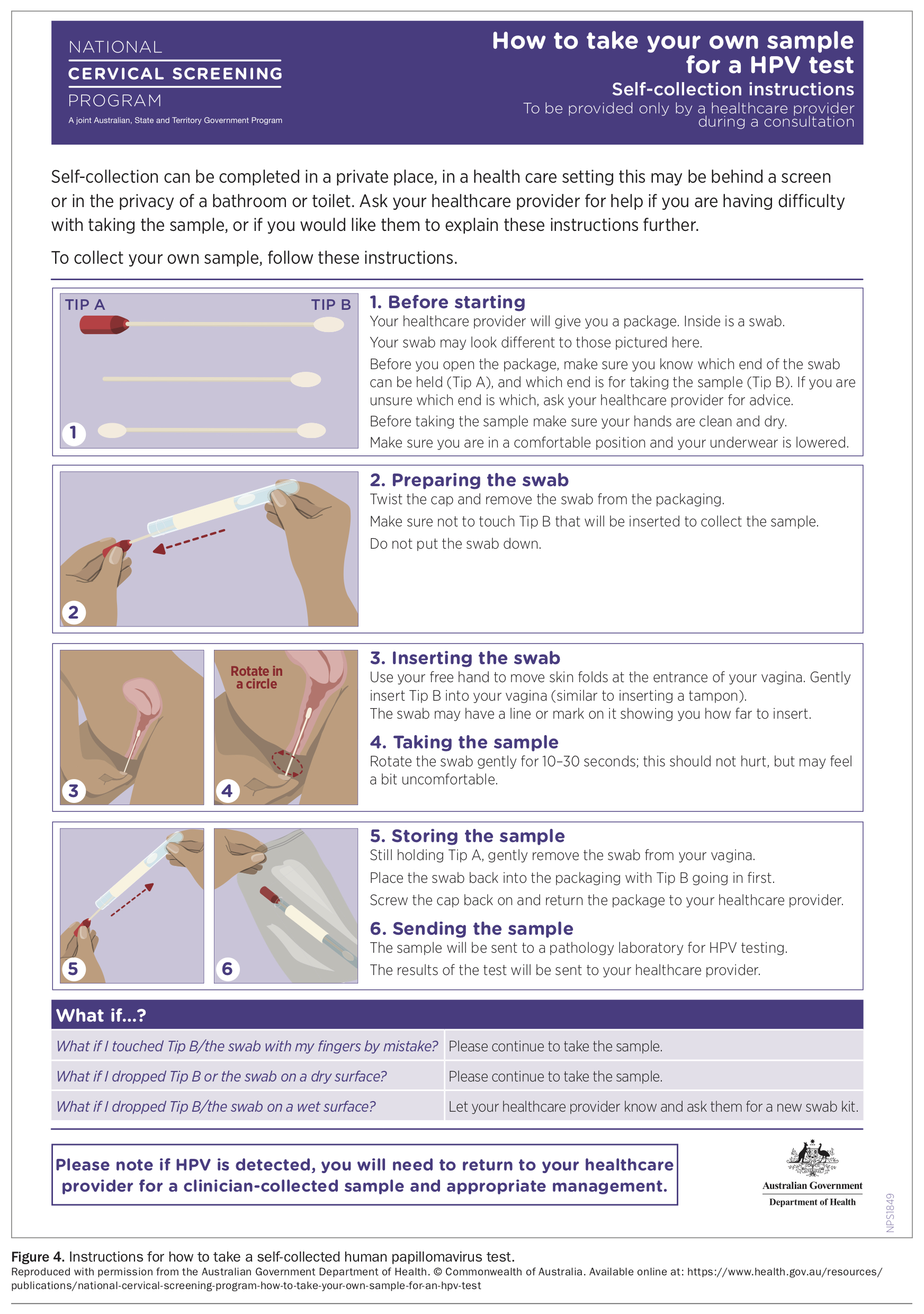
If a patient chooses the self-collection option, instructions about how to take the test should be provided (Figure 4). The person does not have to be observed taking the sample and can choose to take it behind a curtain in the clinic room or in the bathroom. Patients who may have limited mobility, tremor or poor vision can be assisted by the practitioner in the collection of a vaginal swab, which would still be regarded as a ‘self-collected’ vaginal sample. Clinician education and support will be widely available for facilitation of implementation of the updated program, including through Medicine Today.
{kind=link}
Conclusion
The renewed NSCP was implemented in November 2017 and subsequent data collected within the program as well as emergent evidence in relation to HPV testing has resulted in updates to the program and clinical guidelines. The intermediate risk pathway was updated on 1st February 2021 to reflect evidence that participants with persistent HPV (not 16 or 18) infection 12 months after an initial intermediate risk CST are at very low risk of high-grade disease and cancer compared with other groups referred for colposcopy. Guidance was updated in 2018 to clarify the appropriate use of the co-test for women with symptoms, including abnormal vaginal bleeding. In November 2021, the Minister for Health approved universal self-collection as a choice for anyone eligible for routine screening within the NCSP from 1st July 2022. It is hoped that this game-changing strategy will keep Australia on track to become the first country in the world to eliminate cervical cancer by 2035.10 GPs will play an essential role in addressing equity gaps in relation to screening and making elimination of this preventable disease a reality across the many diverse communities in Australia. MT
COMPETING INTERESTS: Professor Bateson and Dr Roeske have received financial support from HealthEd in relation to cervical screening education.