A National Cervical Screening Program update: a guide to self-collection

Professor Bateson is Professor of Practice in the Faculty of Medicine and Health, University of Sydney, Sydney, NSW.
Dr Roeske is a General Practitioner in Melbourne, Vic, and Chair of the Royal Australian College of General Practitioners National Faculty of Specific Interests.
Cervical cancer
Women's health

Since the changes to the National Cervical Screening Program in July 2022, anyone eligible for screening can be supported by their healthcare professional to make an informed decision to have either a clinician-collected cervical sample taken with a speculum or a self-collected vaginal sample. Self-collection of samples for human papillomavirus can help facilitate cervical screening in under-screened and never-screened populations.
On 1 July 2022, a major policy change supporting the choice of either self-collection of a vaginal sample or a clinician-collected cervical sample for primary human papillomavirus (HPV) screening was implemented within the National Cervical Screening Program (NCSP). This change was announced on 8 November 2021 by the former Minister for Health and Aged Care, following recommendations from the Medical Services Advisory Committee after their detailed review of the evidence around the accuracy and acceptability of self-collection.1
Significant advances in our understanding of the pathophysiology of cervical cancer and its association with persistent oncogenic HPV types informed the national school-based HPV vaccination program for 12- to 13-year-old girls, and later, boys, and the shift from two-yearly Pap tests to five-yearly HPV testing within the NCSP in 2017. These initiatives have put Australia on track to becoming the first country in the world to reach the WHO cervical cancer elimination target of less than four cases per 100,000 women by 2028 to 2035.2,3 However, although cervical cancer was the 14th most common cancer in Australian females in 2020, there were still about 933 predicted new diagnoses and 233 deaths, with almost three-quarters of deaths occurring in under- or never-screened people.
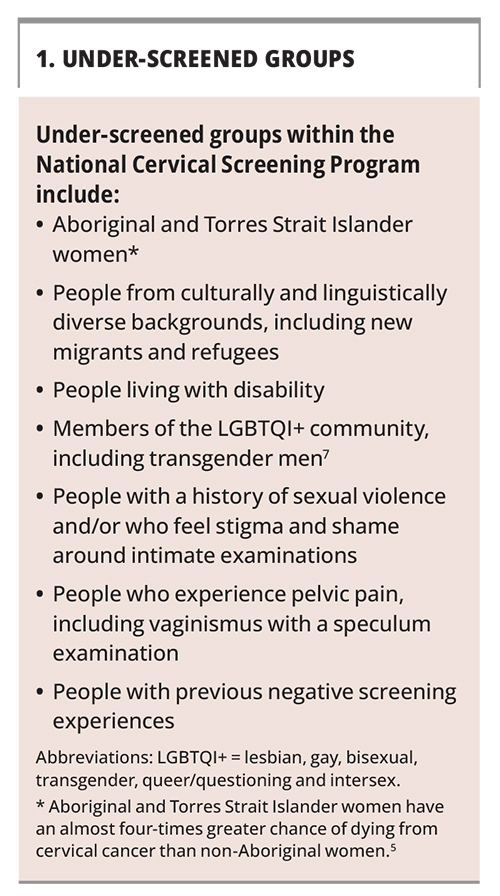
At the end of 2020, more than 30% of people eligible for cervical screening were overdue. Although identification data need to be improved, the limited available data shows that under- and never-screened people belong to multiple and varied groups (Box 1).4-7 The introduction of universal self-collection is a potential game changer in helping to increase participation in the NCSP by these under-served groups and to achieve the elimination goal equitably.
{kind=link}
In this article, we provide practical guidance for clinicians about the changes to the NCSP and how best to support patients in making an informed decision to either have a self-collected vaginal sample or a clinician-collected cervical sample for HPV testing. We also provide links to the guidelines for the management of screen-detected abnormalities in the NCSP (https://www.cancer.org.au/clinical-guidelines/cervical-cancer-screening/management-of-oncogenic-hpv-test-results/self-collected-vaginal-samples) and NCSP resources to support this significant change in clinical practice.
What is self-collection and how accurate is it?
A self-collected cervical screening test (CST) involves the patient taking a sample from the lower vagina with an approved swab, which is sent to the pathology laboratory for polymerase chain reaction (PCR) testing to assess whether any oncogenic HPV types are present. The vaginal swab detects HPV shed from a productive infection at the cervix. An updated meta-analysis published in 2018 showed that HPV testing of a self-collected sample is as accurate as HPV testing of a clinician-collected sample for detecting cervical intraepithelial neoplasia (CIN) 2+ or CIN 3+ when using PCR testing.8 This updated evidence was not available when the renewed NCSP was rolled out in 2017 as previous analyses had used the older, less sensitive signal amplification tests. As a result, before July 2022, self-collection was restricted to people who were aged 30 years or older and were two or more years overdue for screening. Recommendations have now changed and anyone eligible for screening can be supported by their healthcare professional to make an informed decision to have either a clinician-collected cervical sample taken with a speculum or a self-collected vaginal sample.
Self-collection clinical pathways within the NCSP
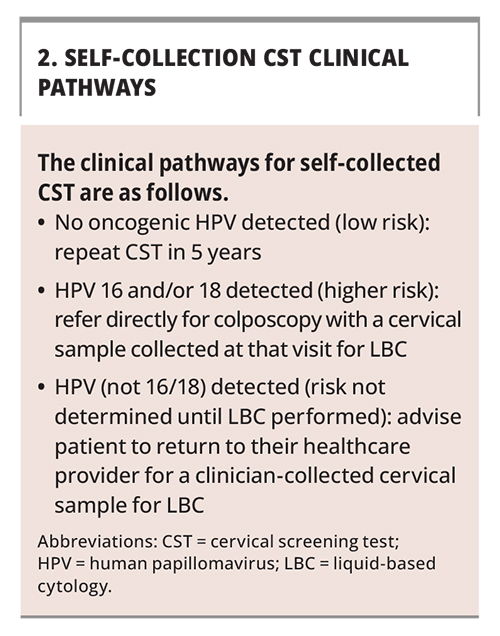
As for a clinician-collected sample, a self-collected sample is used to detect HPV DNA with partial genotyping classifying HPV types into two groups: oncogenic HPV 16 and/or 18, or oncogenic HPV (not 16 or 18) as a pooled result of one or more of these 14 HPV types. However, unlike a clinician-collected sample, a self-collected sample cannot be used for reflex liquid-based cytology (LBC) as it does not contain cells from the cervix. This difference has implications for the self-collection clinical pathways, which must be carefully explained to the patient to support their decision-making process.
The clinical pathways within the NCSP are based on the classification of CST results into low, intermediate or higher risk categories (Box 2). Most patients choosing either self- or clinician-collection will have a negative HPV result and can be safely advised to have a repeat screening test in another five years. In contrast to patients who have a clinician-collected cervical sample and can have reflex LBC performed automatically by the laboratory, patients who have oncogenic HPV (other than types 16 and 18) detected on a self-collected sample are advised to return as soon as is practical for a clinician-collected cervical sample for LBC in order to determine their risk category. This is expected to occur in about 6% of patients who present for routine screening; however, this varies by age – from about 17% in 25 to 29-year-olds to about 3% of people aged 55 years or older.9 To support patients’ informed decision making, it is important to explain about the need to return for a cytology test as soon as is practical if HPV (not 16 or 18) is detected; this can be supported by desktop medical software reminder systems. The presence of higher risk HPV (16 or 18) would be expected in about 2% of patients attending for routine cervical screening. Patients who have higher risk HPV (16 or 18) detected on either a clinician- or self-collected sample should be referred directly to colposcopy. In the case of self-collection, the cytology is performed at the time of the colposcopy consultation. An individual patient’s risk is also based on personal characteristics, including age greater than 50 years, Indigenous status and whether they are overdue for screening. As noted, most patients choosing self-collection will have a negative test result; however, it is likely that this option will be taken up, at least initially, by a greater proportion of those at higher risk, as they may not have undergone screening for many years or ever at all.
{kind=link}
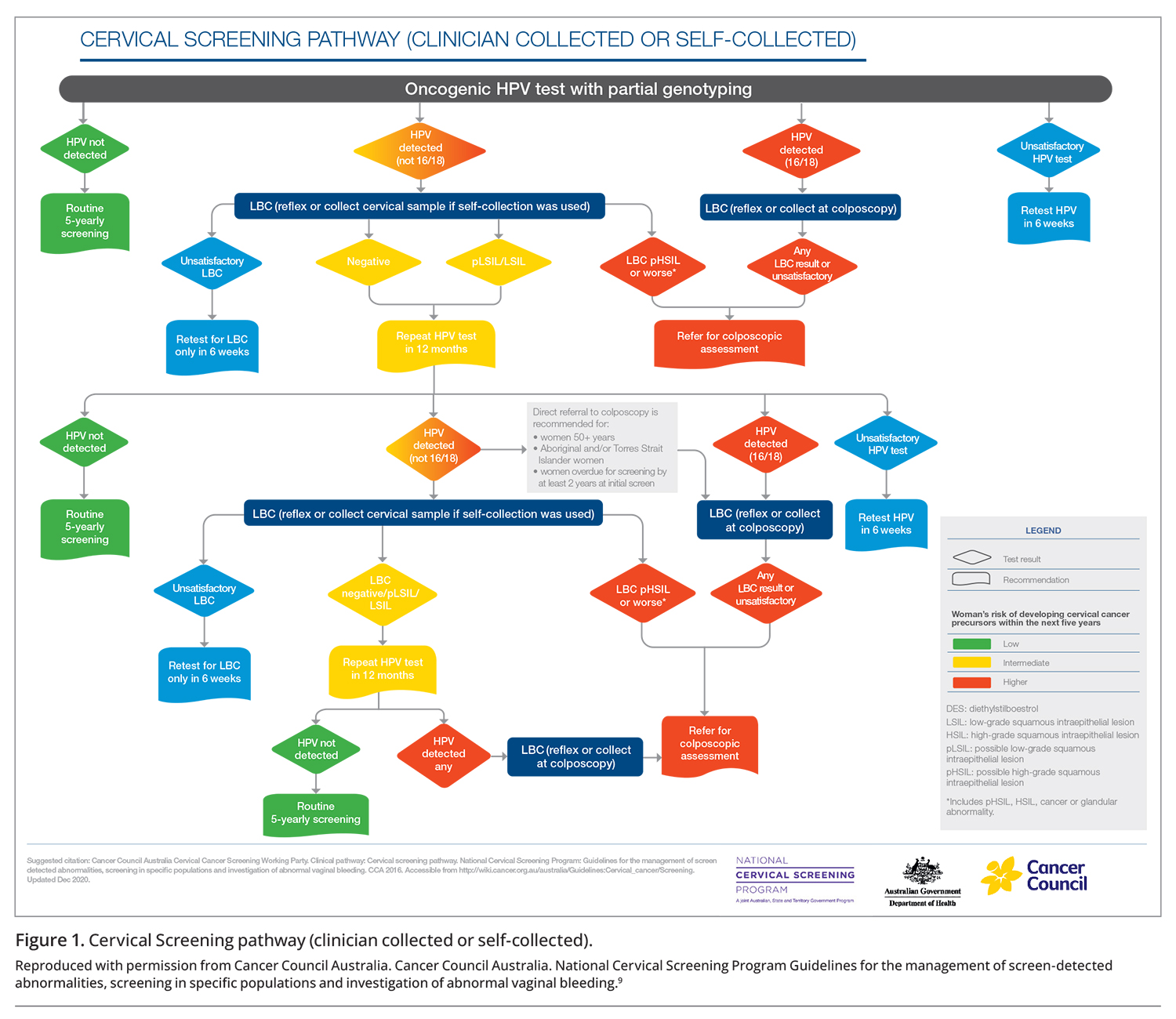
Figure 1 shows the NCSP self-collection low, intermediate and higher risk pathways. It should be noted that self-collected samples for HPV testing are less likely to be unsatisfactory than cytology tests from the cervix and that all HPV assays used for self- collected samples in Australia have a cellularity control, therefore an empty or inadequate sample will not lead to a negative HPV test result. However, there is a very small chance of inhibition of an HPV test in the presence of a large amount of blood (although, in general, if a patient presents during menstruation, the opportunity to offer screening should not be deferred).
{kind=link}
Self-collection: who is eligible and who is not?
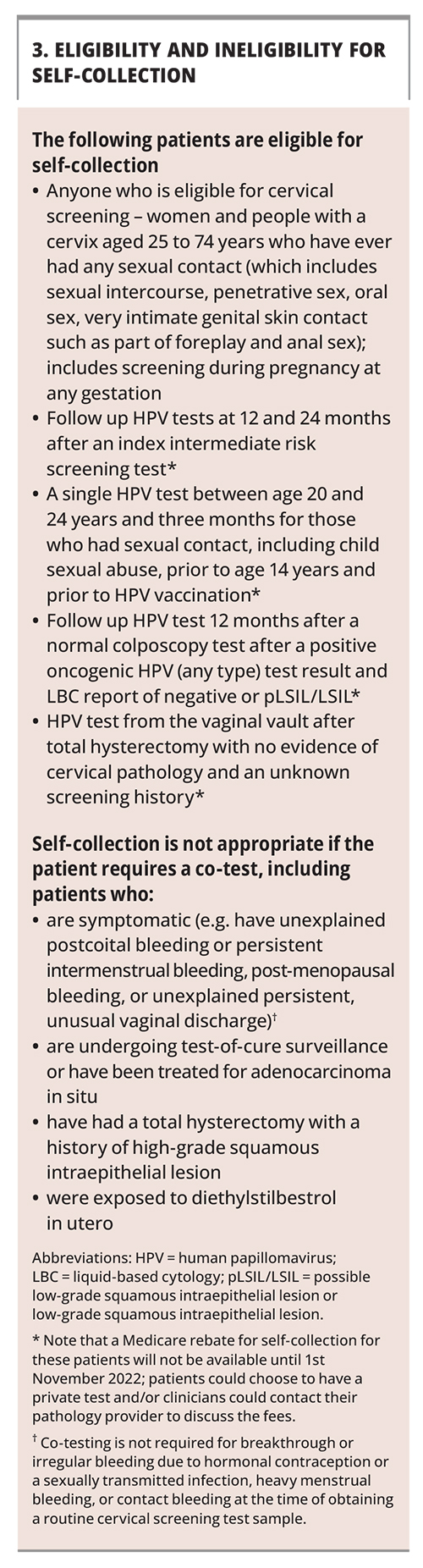
Given that a self-collected sample can be used for an HPV test with partial genotyping but not for cytology, the choice to self-collect should be discussed with anyone eligible for screening or at any point in the pathway where only an HPV test is required. By contrast, anyone requiring a co-test (which involves simultaneous HPV and LBC testing), including patients with symptoms or those deemed at higher risk of harbouring a high-grade lesion of the cervix even with a negative HPV test, are ineligible for self-collection (Box 3).
{kind=link}
Supporting and assisting patients choosing self-collection
The guidelines recognise that patients with oncogenic HPV (any type) detected may require additional and individualised support to progress along the clinical pathway and to access follow up services where they will receive sensitive treatment.9 This can include reassurance and explanation with longer appointments, additional follow up contact and liaison with colposcopy services.
The guidelines also make it clear that there is no requirement to observe the patient collecting their sample and that healthcare professionals can provide assistance if patients have difficulty in taking their own vaginal sample.9 This also includes the clinician collecting the vaginal sample using a self-collection swab without a speculum, which is still classified as self-collection on the pathology request form, and may be useful if, for instance, the patient has low vision, tremor or limited mobility.
Self-collection in pregnancy
Anyone who is eligible for screening within the NCSP aged between 25 and 74 years can choose a self-collected screening test, including at any time during pregnancy. Self-collection of swabs for Group B Streptococcal testing and screening for sexually transmitted infections in pregnancy is routine and safe; similarly, self-collection of an HPV test has also been shown to be safe and effective. Antenatal visits are an ideal time to offer screening to patients who are under- or never-screened, as this may be the only time that some women come into contact with the health system, and these opportunities should not be missed.
Self-collection in the intermediate risk pathway
Self-collection can also be offered in the context of non-screening HPV tests, including for patients undergoing followup HPV testing after an intermediate risk CST (Box 3). The intermediate risk pathway was updated in 2021 in response to emergent evidence that patients with HPV (not 16 or 18) had a very low risk of biopsy-proven high-grade disease of the cervix, and that the vast majority clear the virus within 24 months and many within 12-months.10 Patients with an intermediate risk screening test result requiring a 12-month follow-up HPV test can now choose for this test to be either clinician-collected or self-collected and if, on self-collection, HPV (not 16 or 18) is again detected, the patient will need to return at their earliest convenience for a cytology test to inform the next steps.
Most patients with a persistent intermediate risk result can be safely advised to have a second follow up HPV test in a further 12 months (i.e. 24 months from their index CST), which can also be either clinician- or self-collected. If, at this second follow up, HPV is again detected, a colposcopy referral should be made. However, some groups are considered at higher risk of an underlying high-grade lesion with a persistent HPV (not 16 or 18) result at 12 months even if the LBC result is either negative, possible low grade squamous intraepithelial lesion (pLSIL) or LSIL, and referral for colposcopy is recommended. This includes patients who:
- identify as Aboriginal and/or Torres Strait Islander
- are aged 50 years or more
- are two or more years late for initial CST.
Where can self-collection occur?
The major policy change to offer universal self-collection was driven by the need to reach under- and never-screened people. The guidelines, while stating that self-collection is preferable in a health care setting as this guarantees timely return of the sample, also state that it can occur in any setting that the clinician considers is appropriate in order to support participation of an individual who may otherwise remain unscreened.9
This opens up the possibility of supporting screening via telehealth at home, or at a local pathology collection centre for patients with difficulties accessing clinic appointments or who live in a remote area. Note that when the patient is referred for self-collection to a pathology collection centre after a telehealth consultation, the health care professional must have an arrangement with the laboratory in place to ensure the correct swabs and information to support self-collection are locally available. Critically, in all settings, the requesting clinician takes complete responsibility for informing patients of their results and any required follow up.
Explaining self-collection to patients to support informed choice
It is imperative that the clinician provides clear information about the pros and cons of self-collection versus clinician collection of a CST or follow up HPV test.11 This includes information on how the test will be performed, that a self-collected vaginal sample can only be tested for HPV, and that, unlike for a clinician-collected sample, it is recommended to return for a clinician-collected sample from the cervix if HPV (not 16/18) is detected because cell changes cannot be seen.
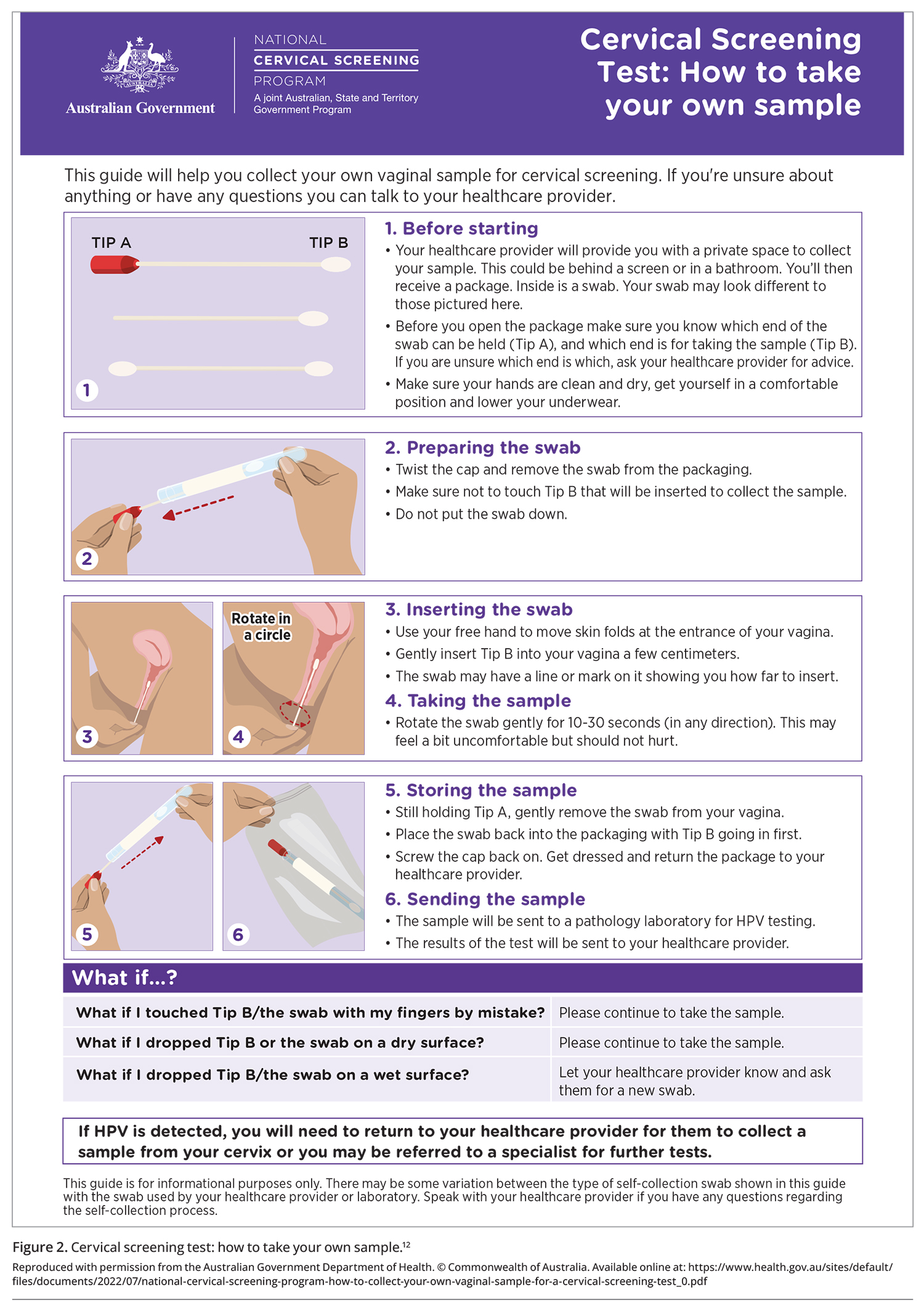
If self-collection is chosen, step by step guidance should be given about how to collect the sample, supported by NCSP resources, including information sheets and instructional videos (www.health.gov.au/ncsp), as well as information on how the results will be received (Figure 2).12 Note that routine genital inspection is not required for asymptomatic patients presenting for a CST but should be performed if symptoms such as vulval pain or a vaginal discharge are present.
{kind=link}
The NCSP portal has multiple resources to support patients and health professionals with co-designed translated materials in 11 languages and six Aboriginal and Torres Strait Islander languages. An online toolkit is available to support under-screened groups, including Aboriginal and Torres Islander people, culturally and linguistically diverse communities, people living with disability and those from the LGBTQI+ community (https://www.health.gov.au/initiatives-and-programs/ncsp-healthcare-provider-toolkit/cervical-screening-options/self-collection-for-cervical-screening).
Using the correct sampling devices and identifying samples as self-collected
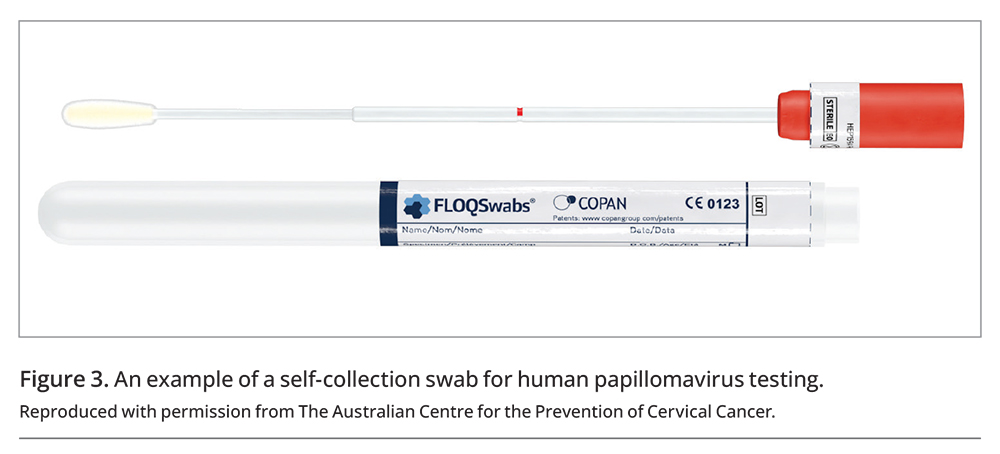
Since July 2022, a range of HPV assays with TGA-approved claims for self-collection have become available. Previously, only three pathology laboratories were offering processing of self-collected samples; however, now several offer this service and more are expected to follow. Some laboratories provide tests that use red-topped flocked swabs, whereas others provide tests that require the swab to be agitated to release cells into a liquid-based medium by the clinician immediately following self-collection (Figure 3). A practical point is to ensure that the swabs are within the printed expiry date, otherwise the pathology laboratory may decline to report the result.
{kind=link}
Healthcare professionals are encouraged to contact their local pathology service to confirm that they can process self-collected vaginal samples, or that they have an arrangement in place to send them on to another laboratory for processing, and to ensure they have the correct swabs, handling requirements and resources to support their patients. Labelling the sample as self-collected as well as providing this information on the pathology request form is essential to ensure the laboratory performs the correct test and provides the correct clinical recommendations. Similarly, write LBC only on the sample and request form for a clinician-collected sample for cytology only after an HPV (not 16/18) test result on a self-collected sample.
Improving identification data and using the National Cervical Screening Register
Identification of under-screened groups within the NCSP is important for supporting initiatives to enhance participation and prevent morbidity and mortality from cervical cancer. In addition to a relevant clinical history, including information on the pathology request form about whether the patient identifies as Aboriginal and/or Torres Strait Islander is essential, as this support accurate data collection as well as impacts on the recommendations provided by the laboratory in relation to the intermediate pathway. Avoiding assumptions regarding a person’s Indigenous status and asking questions directly in a non-judgmental manner is essential. This and other identification information is also important to capture, for those who consent, on the National Cervical Screening Register (NCSR).
The NCSR Healthcare Provider Portal, accessed via a PRODA account, provides timely support through point of care access to the patient’s screening history and also allows health professionals, as well as patients themselves or their nominated personal representative, to update their identification status (https://www.ncsr.gov.au/content/ncsr/en/healthcare-providers/RegisterAccess.html). The NCSR also supports the screening program by sending invitations and reminder letters to participants and has updated information on both its Healthcare Provider Portal and Participant Portal on the option of self-collection. The invitations for people who have turned 25 years old since July 2022, and reminders for people due for their routine five-yearly CST from the end of 2022, also contain information on the option of self-collection.
Conclusion
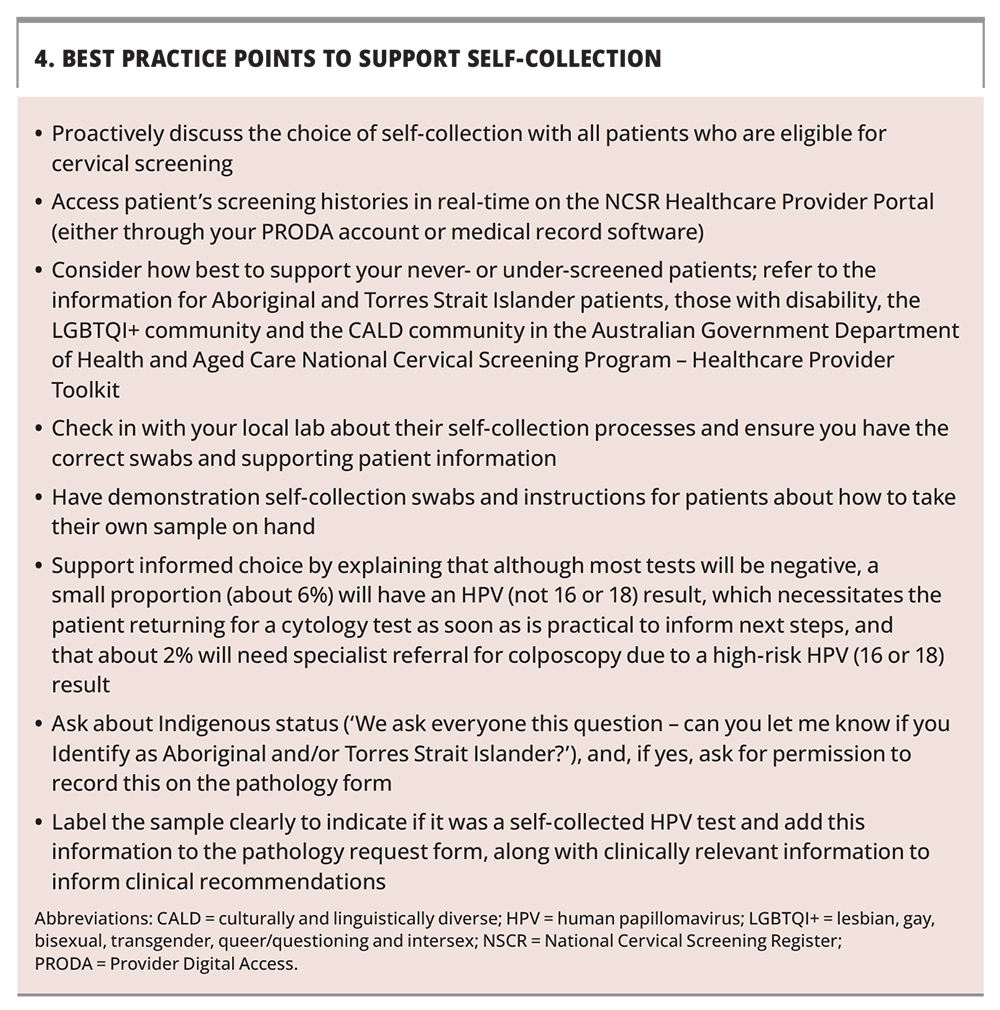
Universal self-collection offers additional choice for participants in the NCSP. By overcoming some of the barriers experienced by groups who are currently under-screened, self-collection plays a key role in supporting a positive and safe screening experience for all. Supporting patients in making an informed choice for either a self- or clinician-collected CST can help overcome inequities in cervical cancer incidence and mortality, and will help ensure that the WHO elimination targets can be reached equitably across Australia. Best Practice Points to support self-collection are listed in Box 4. MT
{kind=link}
COMPETING INTERESTS: Professor Bateson is a co-principal investigator on the Elimination of Cervical Cancer in the Western Pacific program; a Scientific Advisory Board Member for the investigator-initiated trial of cervical screening ‘Compass’, run by the VCS Foundation Australia; Chair of the National Cervical Screening Program (NCSP) Self Collection Implementation Committee; and Co-Chair of the NCSP Quality and Safety Monitoring Committee and has not received payments to herself or her institution for these. Dr Roeske has received payment for attending meetings and/or travel for her involvement in HealthEd/Generation Next, Royal Australian College of General Practitioners, Australian Government Department of Health and Aged Care Cervical Screening Section; payment for participation on the Australian Commission on Safety and Quality in Health Care Cervical Screening Redrafting Working Group; payment for her role as Director of the Royal Australian College of General Practitioners; and has held a voluntary role as Chair of Araluen.