Advanced Parkinson’s disease: a clinical challenge

Advanced Parkinson’s disease is a challenging management problem, with multisystemic motor and nonmotor symptomatology that often manifests in distinct problems, sometimes with opposing mechanisms. Careful consideration of the treatment options, in consultation with a movement disorder specialist, and highly individualised care, involving a multidisciplinary team and appropriate use of ‘device-assisted therapies’ provides the best outcome for patients, improves their quality of life and reduces carer burden and hospital admission rates.
- The course of Parkinson’s disease is highly variable between individuals living with the disease. Some will only ever use oral medications and never require device-assisted therapies.
- Nonmotor symptoms may become dominant in late-stage Parkinson’s disease, and compromised motor treatment to avoid worsening non-motor issues is often needed.
- Device-assisted therapies may be used to obtain more consistent results and avoid unwanted effects of oral treatments.
- Advanced Parkinson’s disease management benefits from a team-based approach, including input from the GP, movement disorders specialists and allied health professionals.
- Device-assisted therapies can improve motor symptoms associated with Parkinson’s disease; however, evidence regarding non-motor symptoms, particularly in advanced disease, is lacking. Therefore, off-label therapies are often used to manage advanced non-motor symptoms.
- Lifestyle management remains as important in late-stage Parkinson's disease treatment as in early disease.
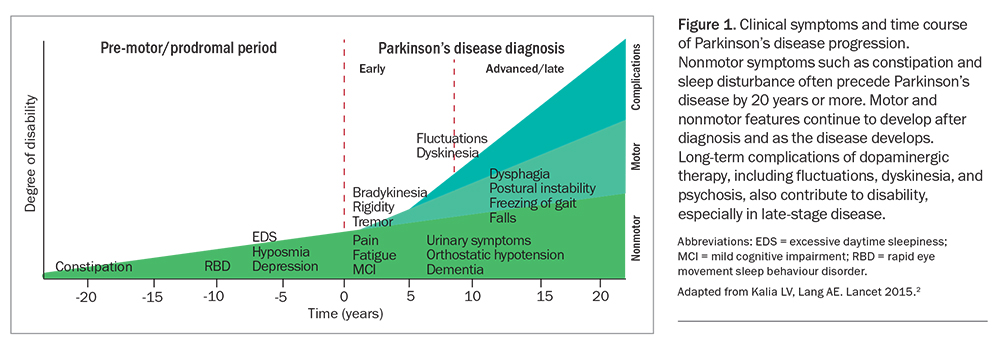
Parkinson’s disease is a common neurodegenerative disorder in Australia and around the world.1 Although the cardinal motor symptoms of tremor, bradykinesia, rigidity and postural instability remain key diagnostic indicators of the condition, we now have a greater appreciation of the systemic effects on nonmotor characteristics including sleep, mood, cognition, autonomic function and bladder, bowel and sexual function (Figure 1).2 Moreover, the symptoms and signs are highly variable between individuals living with the condition.
{kind=link}
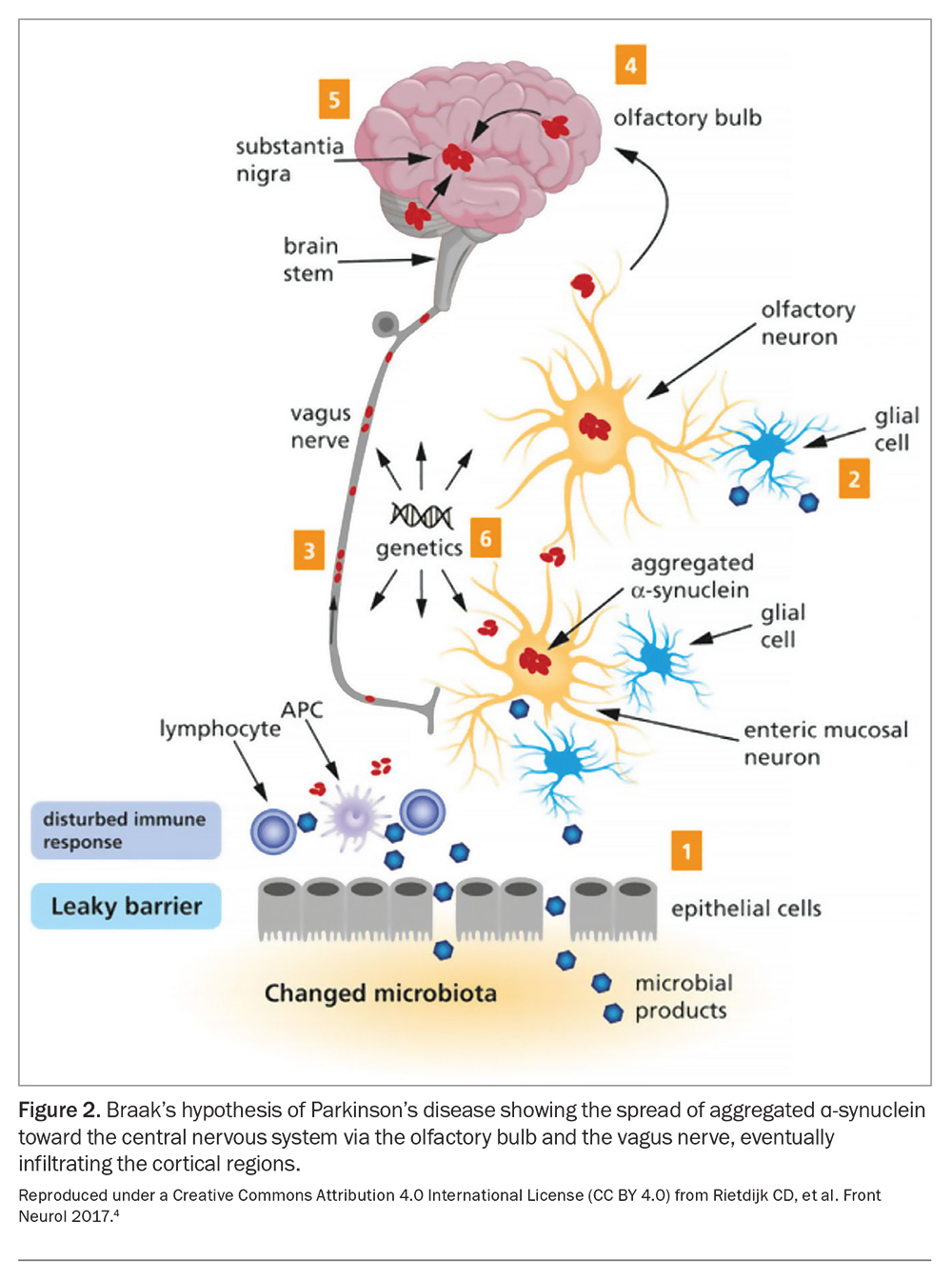
In 2003, neuropathologist Braak and colleagues postulated an infection-like mechanism for Parkinson’s disease, which has led others to propose a prion-like pathological hypothesis of spread. This is a helpful model to explain the early effects on olfaction and constipation, often long preceding the onset of the motor symptoms, with alpha synuclein pathology migrating from extracranial sites to the brain (Figure 2).3-5 This spread and the development of neuronal Lewy body pathology continues throughout the patient's life, and the location, speed and extent of this spread (also ‘staged’ by Braak6) likely contributes to the changes seen both in their symptoms and response to treatment.
{kind=link}
This article focuses on the management of the patient with Parkinson’s disease at a more advanced disease stage. An excellent (and still current) exposition of treatment of early Parkinson’s disease has been published in the January 2015 Medicine Today.7
Defining advanced Parkinson’s disease
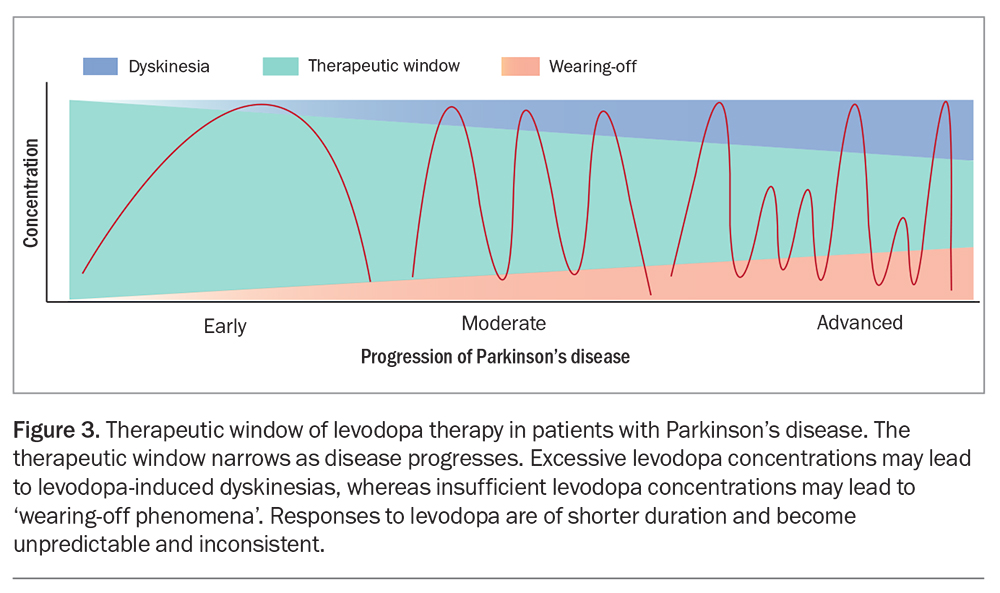
There is a wide ‘therapeutic window’ for treatment in early Parkinson’s disease such that patients with milder disease, and especially younger patients, respond relatively well to ‘some treatment’ (Figure 3). The exact treatment dose requires optimisation but the specific choice of agent and timing of administration is of lesser importance than in later disease.8
{kind=link}
Even in early disease, some medications are more potent than others, with levodopa the preferred option for most patients because of its efficacy. Other agents may have distinct benefits despite overall weaker effects on motor symptoms and signs. For example, dopamine agonists may boost motivation and mood, while also having beneficial motor effects. They are also available in long-acting preparations, such as extended-release pramipexole or rotigotine patches. The latter also avoid issues with gastric absorption. Even less potent agents have their place in treatment and include drugs that block enzyme-mediated destruction of dopamine and other monoamines, such as the monoamine oxidase (MAO-B) inhibitors, rasagiline and safinamide, which are both long-acting and cause relatively few adverse effects.
Historical concerns over early and long-term use of dopaminergic agents have proven to be ill-founded: the complications of dopaminergic therapies are related to the combination of disease duration and severity and drug dosage, rather than the simpler notion of a ‘time-limited’ benefit for the use of any particular agent. Therefore, using multiple agents at lower doses appears to be a more effective and better tolerated strategy than employing monotherapy at a levodopa equivalent dose.
Advanced motor symptoms
Disease progression and the consequent demand or requirement for higher drug dosages leads to complications, including:
- increased side effects of medications
- apparent ‘dose failures’ when individual dose administration is only partially effective (or completely ineffective)
- prolonged periods of feeling ‘off’, which can result in increased motor symptoms of tremor, bradykinesia and rigidity
- motor fluctuations with delayed ‘on’ periods and wearing off before the next dose is due
- disabling dyskinesia, which may be choreiform and hyperkinetic at ‘peak dose’ plasma levels or painful and dystonic as medications wear off
- new-onset gait freezing, which has an inconsistent response to dopaminergic treatment
- more significant nonmotor symptoms, such as psychiatric or psychological effects including anxiety, dyspnoea and mood effects.
Advanced nonmotor symptoms
Nonmotor symptoms increase in their prevalence and impact with disease progression, such that they may become dominant in determining patients’ quality of life and therefore choice of therapy.9 Disordered autonomic nervous system function is common in advancing Parkinson’s disease. This dysautonomia may lead to sleep disruption due to failure in thermoregulation and bladder detrusor instability. Constipation is almost universal and sialorrhoea is a common complaint in patients with advanced Parkinson’s disease. Orthostatic hypotension is also common and can result in falls. Dopaminergic therapies may exacerbate diurnal somnolence, hypotension and other symptoms. Obstructive sleep apnoea is more frequent in those with Parkinson’s disease. Problems with speech and swallowing and the impact of severe constipation can cause faecal impaction, pain, anorexia and even heighten the risk of aspiration pneumonia, resulting in significant morbidity and mortality and high rates of hospital admission.
Although present in early disease, cognitive impairment impacts more significantly on patients with advancing age and longer disease duration. Hallucinations and psychosis can occur, even when results of cognitive impairment on tests more suited to detecting the amnestic signs (e.g. Alzheimer’s pathology) are only minimally abnormal.
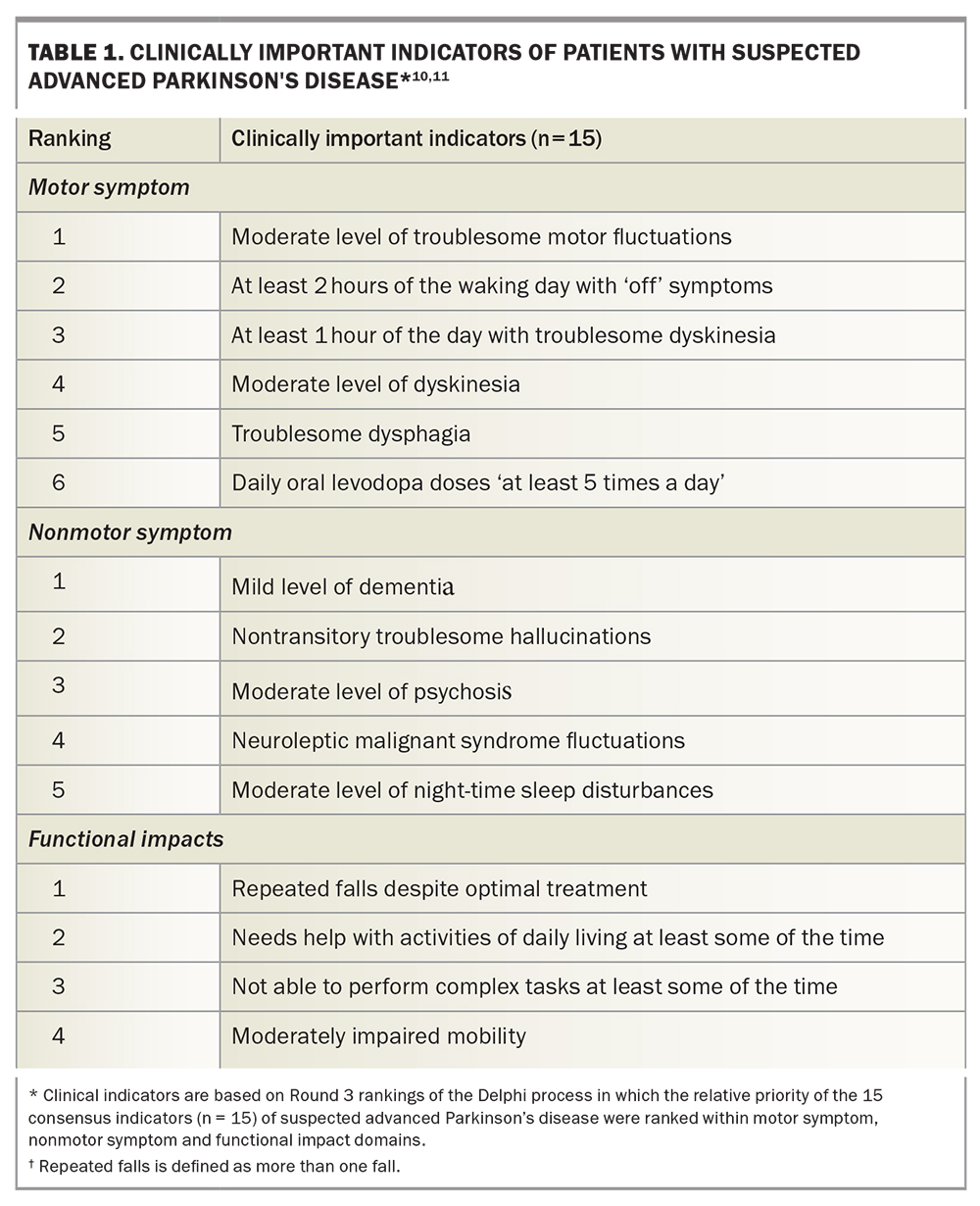
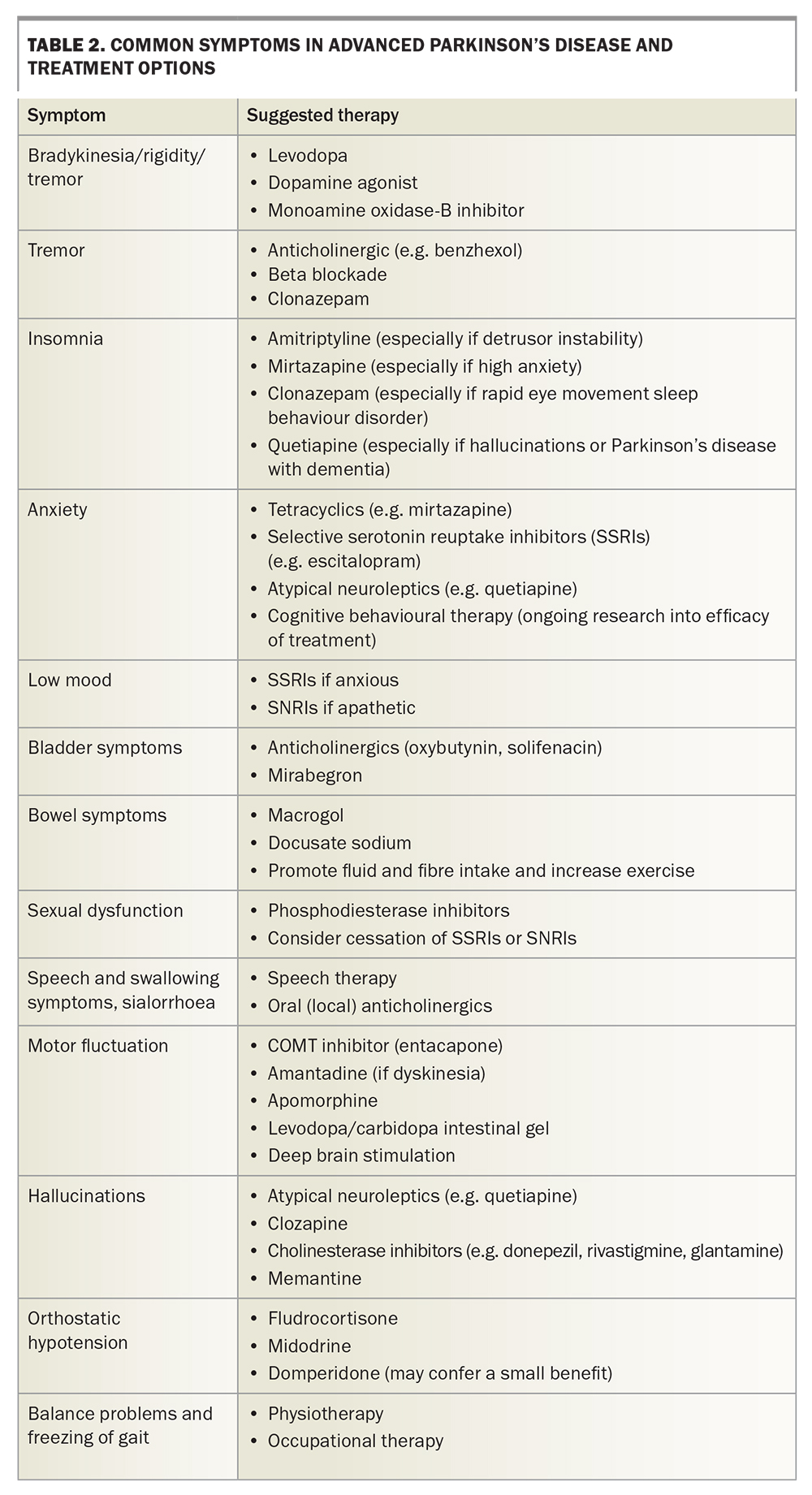
Delphi techniques have been used to come to a consensus view from international experts on the definitions of advanced Parkinson’s disease and hallmark the issues considered most important in identifying the condition (Table 1).10,11 Once identified, advanced Parkinson’s disease may indicate the need to consider device-assisted therapies. Common symptoms of advanced Parkinson’s disease are summarised in Table 2.
{kind=link}
{kind=link}
Treatment in late-stage Parkinson's disease
One of the main challenges in managing patients with advanced Parkinson’s disease is the conflicting treatment requirements of the different symptoms. For instance, optimal treatment of motor symptoms may provoke nonmotor complications, such as hallucinations, psychosis, orthostatic hypotension and diurnal somnolence. Reducing pharmacotherapeutic burden or improving the consistency of drug delivery may, however, allow dose reduction and optimise benefit without causing added adverse effects.
Lifestyle modifications
It is now generally accepted that exercise has a significant beneficial impact on the health of patients with Parkinson’s disease. Clinical trial evidence is strongest for the benefits of weight resistance exercise, but this may reflect the quality of the trials rather than a specific benefit of the type of exercise used. Ongoing research may prove the (currently anecdotal) benefit of cardiovascular exercise.
An overall healthy diet can reduce the impact of constipation, with high dietary fibre and oral fluid intake specifically having the most benefit. Caffeine has motor benefits in Parkinson’s disease, and a moderate intake has been suggested to reduce the onset of disabling dyskinesia. It also increases alertness and may reduce constipation. However, it is also a detrusor irritant and diuretic, and may worsen urinary symptoms.
Protein competes with the enteral absorption and subsequent delivery of dopamine to the brain. It can therefore can be useful to separate the timing of drug administration from heavy dietary protein loads, especially in patients with more advanced disease. The timing of drug administration in general tends to become increasingly important as the condition progresses.
Weight management is also important. Being overweight increases the impact of impaired balance, further slows walking speed and worsens the effects of comorbid pathologies such as osteoarthritis and sleep apnoea. Conversely, low bodyweight and poor appetite can be problematic in more elderly patients, many of whom struggle to maintain muscle mass. Large fluctuations in weight can have significant impact on drug dosages and may lead to either undertreatment or toxicity if such weight changes go unacknowledged.
Multidisciplinary care
Ideally, patients with Parkinson’s disease should be under the care of a multidisciplinary team, which includes a physiotherapist, an exercise physiologist, a speech and language therapist, a movement disorder specialist and a neuropsychologist, co-ordinated and comanaged by their GP. Medicare supports the use of such a team, with the provision of funding for allied health practitioners after the patient’s GP makes a Management Plan and Team Care Arrangement. These plans facilitate six-monthly or annual reviews with a GP and provide for Medicare Benefits Schedule (MBS) funding for up to five sessions per year with allied health practitioners. Additional funding may be sought from the National Disability Insurance Scheme (NDIS) in people aged under 65, or from My Aged Care in older patients.
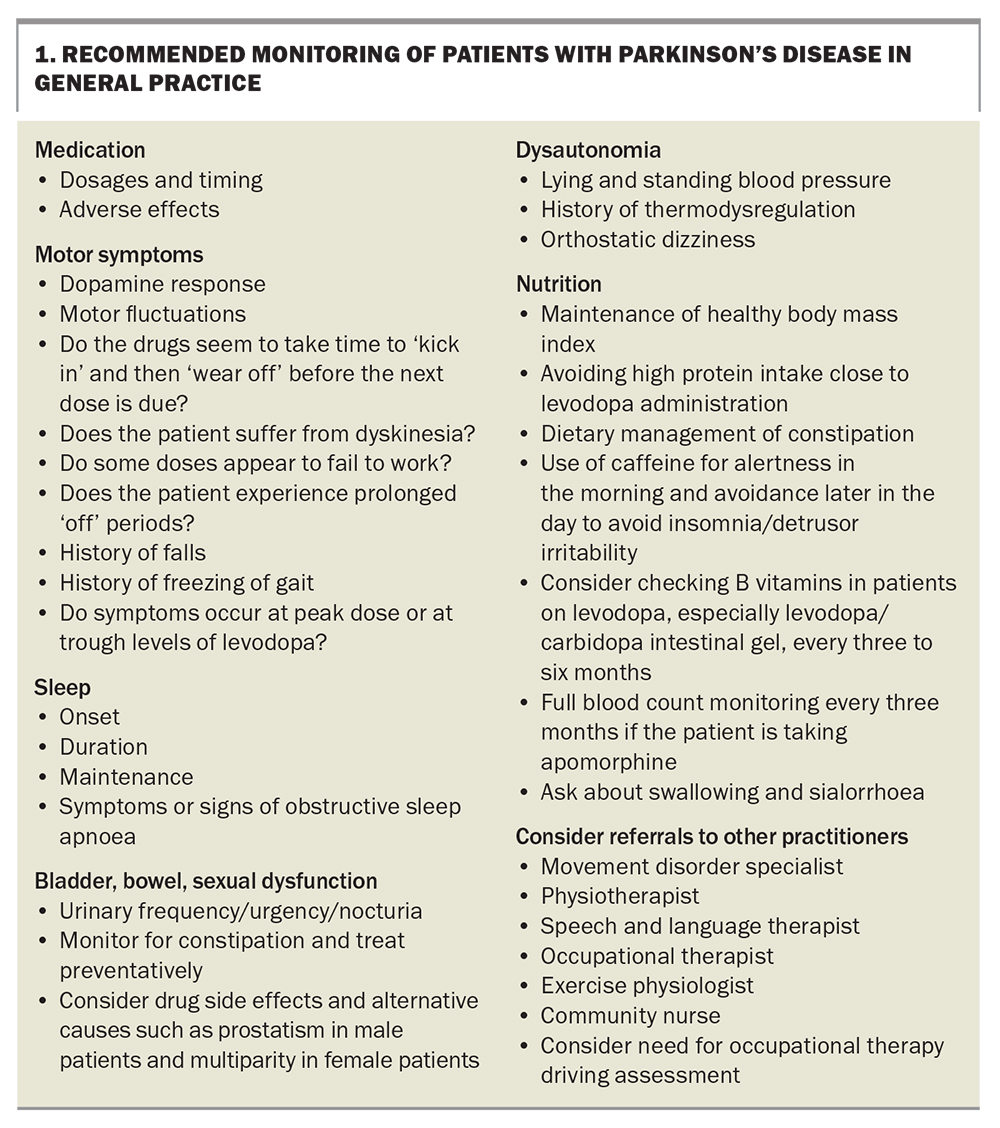
With advanced disease, the input of these health professionals becomes invaluable, especially when medications reach limitations in their utility. Preventing falls and aspiration pneumonia and finding strategies to manage cognitive decline are best achieved with the assistance of a multidisciplinary team. An expert neuropsychiatrist is also a valuable addition to help manage anxiety, mood, sleep and other psychiatric symptoms. In the general practice setting, patients should regularly undergo a medication assessment and be monitored for motor symptoms, sleep, mood, dysautonomia, nutrition and bladder, bowel and sexual dysfunction (Box 1).
{kind=link}
Oral therapies
Despite using the above strategies, some patients eventually begin to develop complications, such as motor fluctuations, disabling dyskinesias, intolerable ‘offs’ (either motor or psychological), dose failures and other symptoms of disease progression. These symptoms can be ameliorated with further oral treatment, including enzyme inhibitors (e.g. catechol-O-methyl transferase [COMT] inhibitors such as entacapone) or the use of additional antiparkinsonian agents such as amantadine, which is an effective antidyskinetic agent. Unfortunately, amantadine may be poorly tolerated in older patients, often causing peripheral oedema, hallucinations and confusion.
Dopaminergic drugs may also prove problematic. In seeking the best motor and psychological ‘on’, some patients may overadminister their medications and develop addictive or dependent behaviours (known as ‘dopamine dysregulation’). Sudden withdrawal of dopamine agonists can also cause dopamine agonist withdrawal syndrome. Even in the most resilient patient, however, the oral adjuvant approach may afford only a temporary ‘stay’ of symptoms, which then require a more involved approach in the form of a device assisted therapy.
Device-assisted therapies
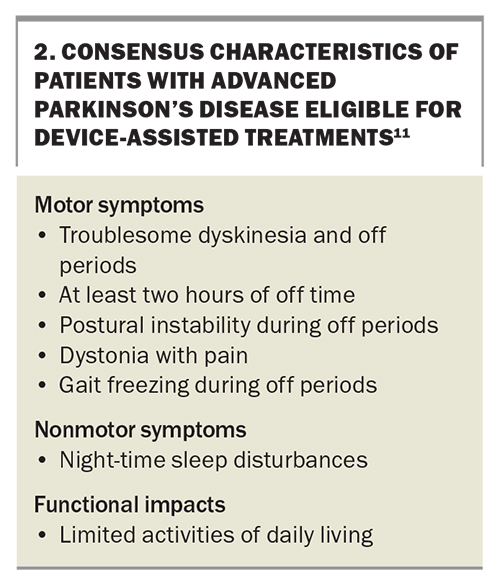
Three main device-assisted therapies are currently available for patients with advanced Parkinson’s disease: apomorphine, levodopa/carbidopa intestinal gel and deep brain stimulation. All three require referral to a movement disorder specialist, both for their expert input and to enable PBS subsidy or MBS funding. Although prescribing these devices is not limited to specialists, patients usually stay in a movement disorders speciality clinic for ongoing care, to be monitored for drug dosages and for device programming. Seven key consensus characteristics are associated with patients with advanced Parkinson’s disease who are eligible for device-aided treatments (Box 2).11
{kind=link}
Ideal care requires constant dialogue between the treating GP, who is often able to see the patient more frequently and may be more knowledgeable about the patient’s social circumstances and other medical issues, and specialist and allied health providers. Furthermore, most patients do best when supported by a caregiver, who may have greater dexterity and cognitive ability, to manage devices and associated paraphernalia. GP input is invaluable in promoting lifestyle modification and strategies, encouraging and ensuring ongoing referral to specialist and allied healthcare practitioners and providing another source of education for patients and their families on living with Parkinson’s disease.
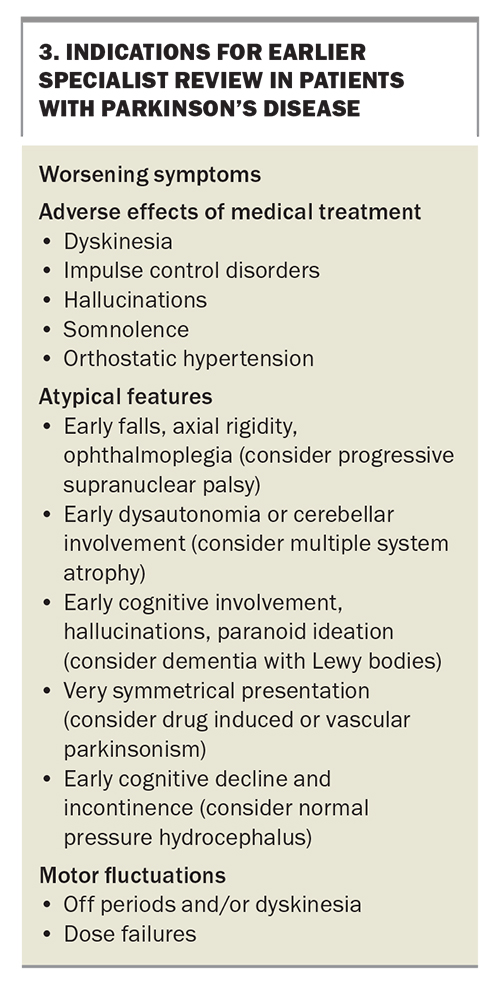
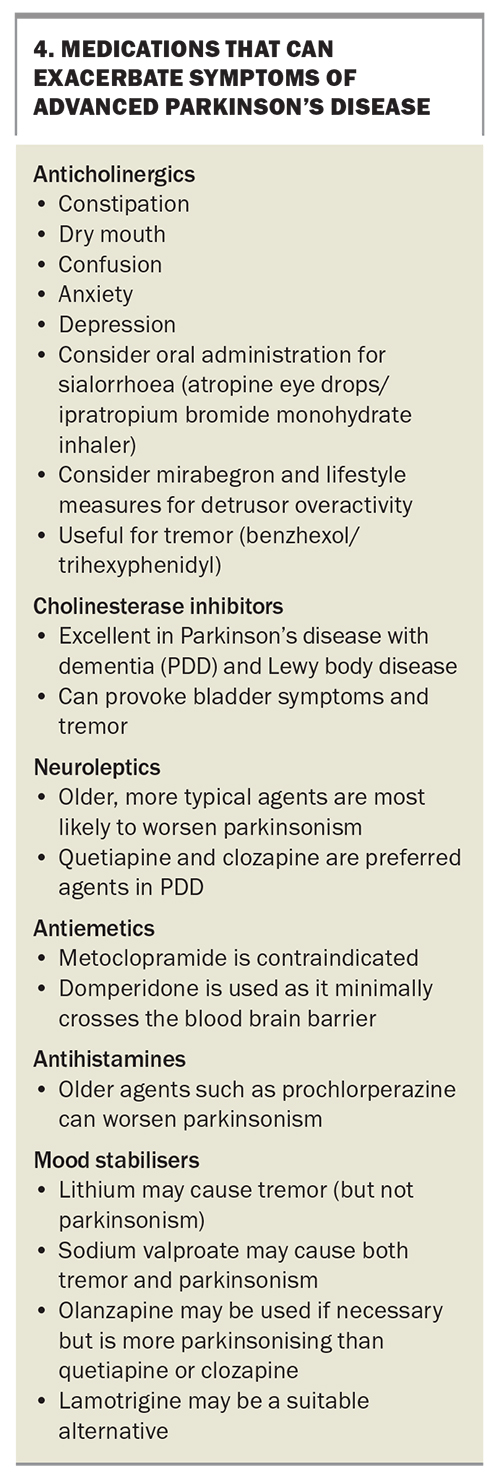
Regular contact with a GP also facilitates more urgent specialist review, if needed, to consider escalating treatment. Indications for early specialist review for patients with Parkinson’s disease are listed in Box 3. After such specialist appointments, GPs are often the first ‘port-of-call’ for adverse effects arising from changes in drug treatment or dosage (Box 4). Knowledge of these adverse effects and how best to manage them allows timely alternative treatment to be tried in between specialist reviews.
{kind=link}
{kind=link}
Apomorphine
Apomorphine is a dopamine agonist that is structurally related to morphine but markedly different in its pharmacological effect. This drug enables the least invasive of the currently available device-assisted therapies. Used as an emetic agent in veterinary practice, it requires prophylactic antiemetic therapy before starting treatment in humans, usually with domperidone (which does not significantly cross the blood brain barrier, unlike metoclopramide, which should not be used in Parkinson’s disease because of central dopaminergic effects). Both needle phobia and nodule formation from repeated administration can be barriers to use; however, thus far, other modes of administration such as a ‘sublingual film’ remain unavailable.
Apomorphine is available in a pen device for intermittent (as required) use, such as when dose failures occur or as a rapidly effective ‘top-up’ therapy for unpredictable ‘off’ episodes. It is also used as a continuous subcutaneous infusion, facilitated by modern electronic pumps that allow variable rates and ‘extra-dose’ administration.
Although, as with other dopamine agonists, impulse control disorders are a theoretical risk, more frequently encountered side effects of apomorphine include dyskinesia, somnolence, peripheral oedema, skin reactions (including nodule formation) and, rarely, bone marrow dysfunction. The latter requires regular monitoring of the full blood count every three to six months.
Levodopa/carbidopa intestinal gel
Levodopa/carbidopa is usually administered as a tablet, both as immediate-release and slow-release preparations. Neither preparation significantly avoids the issues of variable gastric emptying and intestinal absorption, which are compounded by the effects of dietary protein, as mentioned earlier. To minimise adverse effects, levodopa/carbidopa intestinal gel (LCIG) is administered into the small intestine, either through a nasojejunal tube (as a trial of therapy) or via a percutaneous gastrostomy and jejunostomy (PEG/J) tube, which has a gastric tube through which an inner jejunal extension is passed.
Few specific side effects of LCIG are seen, other than those encountered already with the tablet, but the tube and gastrostomy site need careful management to avoid infection and erosion or granulation tissue formation. LCIG is associated with peripheral neuropathy, perhaps due to malabsorptive effects on B vitamin levels. Patients should therefore be warned of this potential adverse effect in advance and their B12 and B6 levels monitored every three to six months.
Siting the PEG/J tube is often achieved through a brief hospital admission during which a nasojejunal tube trial of therapy is first completed. However, recent national and international experience (accelerated by the COVID-19 pandemic) suggests that the nasojejunal phase is superfluous, and that tube placement could be done as a routine day procedure in the endoscopy unit and subsequent dose titration achieved by community nurses with movement disorder specialist supervision.
Complications of LCIG are patient-specific, with managing the stoma more problematic in patients with high body mass index or poor personal hygiene. Even with optimal care, in some patients, the ‘foreign body’ of the PEG/J tube leads to erosion of tissue and presents a risk of chronic granulation tissue formation and infection. Furthermore, patients with dopamine-dysregulation syndrome have an incredible talent for finding the ‘unlock’ codes to their pumps to enable additional dose administration.
Deep brain stimulation
Functional neurosurgery is the most invasive way to routinely manage Parkinson’s disease and is seen as a last resort by many people with the condition. However, there is evidence that early deep brain stimulation (DBS) affords long-term benefits, and trials are underway to look for a disease-modifying benefit.12
For medically refractory tremor (Parkinson’s disease-related and otherwise), DBS is an excellent and well tolerated therapy, and outperforms the other device-assisted therapies. For patients with tremor-dominant disease, some centres have advocated for the use of traditional tremor ‘targets’, including the ventral intermediate nucleus of thalamus, caudal zona incerta and posterior subthalamic area (dentatopallidorubral tracts). However, since nontremor motor symptoms may later manifest, even in patients who are tremor-dominant in early disease, most centres favour the subthalamic nucleus (STN) as a therapeutic target. The internal nucleus of the globus pallidus (GPi) is a reasonable alternative target, especially when indicated by severe dyskinesia or where STN targeting might be contraindicated due to pre-existing dysarthria or high psychiatric risk.
DBS has a similar efficacy to the ‘pump therapies’ (described above) in managing dyskinesia, motor fluctuations and dose failures. No blinded ‘head-to-head’ comparisons exist between therapy types, however, so this evidence relies on trials using differing patient populations and observational reports.
Adverse effects of DBS include immediate surgical risks, such as complications of the surgery (e.g. intracranial haemorrhage) or anaesthesia, and the risk of nonideal DBS lead positioning and subsequent impairment of treatment response or adverse effects. Careful stereotactic planning, intraoperative neurophysiological recordings and test stimulation (in the awake surgical patient) reduce the risk of misplacing leads, but do not completely obviate the risk of unwanted stimulation effects. These include deleterious effects on speech, balance or other motor effects, which are often immediate and easily detectable. Conversely, changes in mood or personality, which are not easily detected, may only become more apparent over time. Patients undergoing DBS, therefore, require careful and frequent follow up, especially in the immediate postoperative period.
The major advantage of DBS over other functional surgical techniques is the ability to adjust the stimulation – both the basic physical parameters (such as potential difference [voltage], current, pulse width and frequency) and the precise location of stimulation using DBS leads with multiple electronic contacts. This enables optimisation of the treatment effect, minimisation of side effects, and titration of the treatment against reduced drug dosages and disease progression. Moreover, recent technological advances allow remote programming (with internet-based video telehealth) and some sensing capability, with the ability to record brain signals from patients with suitable implanted devices.
Other functional neurosurgical techniques
Before DBS was developed, traditional lesioning techniques created permanent damage, often to similar neurosurgical targets as DBS, in the subcortical nuclei of the brain. More recently, other noninvasive image-guided techniques have been developed to afford functional neurosurgical benefits to patients who are medically unsuited to undergo neurosurgery.
Magnetic resonance-guided focused ultrasound (MRGFUS) is the most recent of these lesioning approaches, with dedicated machines in centres in Sydney and Melbourne, and plans for another to be installed in the Gold Coast. Thus far, many referrals to these centres have been for patients who were later deemed better suited to DBS. The lack of post-procedural adjustability, reluctance to treat bilaterally (especially for fear of causing balance issues), and the lack of current Medicare rebates have negatively impacted the use of MRGFUS. It is more frequently used in essential and other tremor disorders in patients who are not thought suitable for DBS. Gamma knife radiosurgery is another lesioning technology used to manage movement disorders.
Limitations of lesioning techniques include the inability to modify the effect once the treatment is complete, and the high risk of balance issues necessitating that most patients only receive unilateral treatment. Nevertheless, for patients for whom DBS or pump therapies are unsuitable, especially those with tremor-dominant disease, these techniques offer a safer, less invasive alternative.
Future device-assisted therapies
Levodopa/entacapone/carbidopa intestinal gel
Levodopa/carbidopa/entacapone is currently available as a combined tablet or capsule. A gel formulation is approved for intestinal tube administration, akin to LCIG.13 Whether the addition of entacapone confers a significant additional benefit over continuous LCIG administration remains to be seen.
Subcutaneous levodopa infusion
A subcutaneous infusion of levodopa/carbidopa is in the clinical trial phase of development. Like apomorphine, it may offer a less bulky and invasive alternative to intestinal gel treatments; however, needle phobia and injection site reactions may be barriers to use.14
Management of nonmotor symptoms
As Parkinson’s disease progresses, the relative importance and burden of nonmotor symptoms can significantly increase and often supersede motor symptoms in their impact on quality of life.15
Dysautonomia
Orthostatic hypotension (OH; a postural drop of ≥20 mmHg systolic or ≥10 mmHg diastolic) is a significant cause of falls and other symptoms in late-stage Parkinson’s disease. It also causes light-headedness, dizziness, blurred vision and ‘coat-hanger pain’. Neurogenic OH is also associated with ‘reverse dipping’ (relative high blood pressures at night) and supine hypertension, and can pose challenges in choosing when and with what to medicate. Twenty four-hour blood pressure monitoring is superior to self-measurement in determining the true need for treatment, and can serve to highlight symptoms such as hypotension after levodopa dosing or meals.
OH can be managed by encouraging recumbent physical activity and slower transitions from supine to standing. Smaller, more frequent meals and increased fluid intake are also helpful. Compression stockings can be used, but are difficult for patients to put on.
After cessation of any antihypertensive agents and anticholinergics, treatment can be instituted with droxidopa, pyridostgmine, fludrocortisone or midodrine. Droxidopa is not currently available in Australia, and midodrine can be difficult to source and fund. There may be a small additional benefit from domperidone. Supine hypertension may require management with antihypertensive therapy at night.
Bladder dysfunction is experienced as both urinary urgency and nocturia. Infectious and outflow causes must be excluded and urology referral is recommended, especially in men to exclude possible prostatic causes. Management of fluid intake in the evening can reduce nocturia, and other simple measures can be taken to manage daytime urination frequency. Solifenacin is recommended for detrusor overactivity; however, because it is expensive, oxybutynin or mirabegron (the latter used when anticholinergic effects need to be avoided) are often used. Cotreatment for prostatic hypertrophy with alpha-adrenergic antagonists and 5-alpha reductase inhibitors may also worsen or provoke OH. Botulinum toxin can be used to manage severe cases of detrusor instability.
Constipation is common in Parkinson’s disease and almost universal in advanced disease. Again, it is important to exclude alternative causes. Fibre from dietary fruit and vegetable intake and olive oil intake are helpful, as are physical activity and adequate hydration. Both probiotics and prebiotic fibre have level 3 trial evidence. Macrogol, lubiprostone and prucalopride are reasonable laxative agents, with macrogol being the most readily available and frequently used. Psyllium husk, lactulose and stimulants laxatives (e.g. senna) have a role but can cause issues in the dehydrated patient.
Sialorrhoea (drooling)
Sialorrhoea not only impacts quality of life and causes embarrassment, it can increase the risk of aspiration and pneumonia. It is predominantly caused by reduced swallowing, complicated by facial bradykinesia. Simple measures such as chewing gum can increase swallowing frequency. Glycopyrrolate is profoundly anticholinergic, and, although effective in reducing salivation, can cause excessive dryness, worsen constipation and have cognitive side effects. Instead, topical (orally administered) anticholinergics, such as sublingual atropine (eye) drops or ipratropium sprays, are often used. Botulinum toxin injected into the parotid and submandibular salivary glands can be effective but may increase the risk of dental caries and is seldom used for sialorrhoea in Parkinson’s disease.
Pain
Pain is prevalent in people living with Parkinson’s disease and increases with disease progression. Parkinson’s disease often amplifies underlying sources of pain, such as comorbid arthritis or neuropathy, and causes painful dystonia in challenging areas, such as the trunk and abdomen, where more sinister causes must first be excluded. Conservative measures including stretching, massage and bathing, yoga and exercise, have been suggested to help with pain management. Pharmacological management, especially with opiates, must be judiciously weighed against the risks of side effects, particularly on constipation and cognition. For this reason, NSAIDs, particularly COX-2 inhibitors, may be used in preference. Maintaining adequate dopaminergic therapy may be helpful, even with lower-potency agents such as safinamide and COMT inhibitors. Gabapentin, pregabalin and duloxetine may help with centrally-mediated or peripheral neuropathic pain.
Sleep
Both night-time insomnia and excessive daytime sleepiness can be problematic in late-stage Parkinson’s disease. Good sleep hygiene is vital and should be reinforced with patients, family members and carers. Obstructive sleep apnoea occurs at increased rates in people living with Parkinson’s disease and should be treated accordingly.
Drugs that promote alertness, such as amantadine, selegiline and selective serotonin reuptake inhibitors, should be restricted to being taken at the beginning of the day. Preventing ‘wearing off’ effects overnight with long-acting agents, such as controlled release levodopa preparations and long-acting dopamine agonists including topical agents (e.g. rotigotine), and managing detrusor instability may reduce night-time waking episodes. Dopaminergic agents can be sedating, which can be beneficial for night-time insomnia but can provoke diurnal somnolence. Dopamine agonists are particularly prone to causing somnolence and triggering ‘microsleeps’ that may create risks for driving, especially in tandem with obstructive sleep apnoea. Higher doses of dopamine can be paradoxically alerting through actions on post-synaptic receptors. Both melatonin and zopiclone are listed as ‘possibly useful’ by the Movement Disorder Society Task Force on Evidence-Based Medicine.
Low-dose clonazepam is often successfully used to treat rapid eye movement sleep behaviour disorder. There is some evidence of a role for melatonin; however, effective treatment may require higher doses than are routinely available with PBS subsidy in Australia.
Anxiety
Patients with Parkinson's disease often experience anxiety related to wearing off effects. Increasing dopaminergic treatment may ameliorate these symptoms. Otherwise, both selective serotonin reuptake inhibitors (SSRIs) and serotonin and norepinephrine reuptake inhibitors (SNRIs) can be useful. Cognitive behavioural therapy is currently the subject of ongoing research. Apathy is clinically challenging to differentiate from the effects of immobility or mood; however, there is some evidence for behavioural approaches and pharmacotherapy using rotigotine and rivastigmine in treating apathy.
Hallucinations and psychosis
Hallucinations and delusions may complicate late-stage Parkinson’s disease and Parkinson’s disease dementia. Cessation of provocative agents (e.g. dopamine agonist) is recommended before trialling low-dose antipsychotics. In sequence, anticholinergics, monoamine oxidase inhibitors, amantadine, dopamine agonists and catechol-O-methyl transferase inhibitors should be ceased, with levodopa reduction as a last resort. Quetiapine and particularly clozapine appear less likely to provoke worsening of motor symptoms compared with older or more typical neuroleptics when used to reduce hallucinations or paranoid ideation. Only clozapine and pimavanserin have a scientific evidence base for efficacy in reducing hallucinations. However, the clozapine requires referral to an amenable psychiatrist and subsequent monitoring in a clozapine clinic, and pimavanserin is not available in Australia.
Cognitive decline
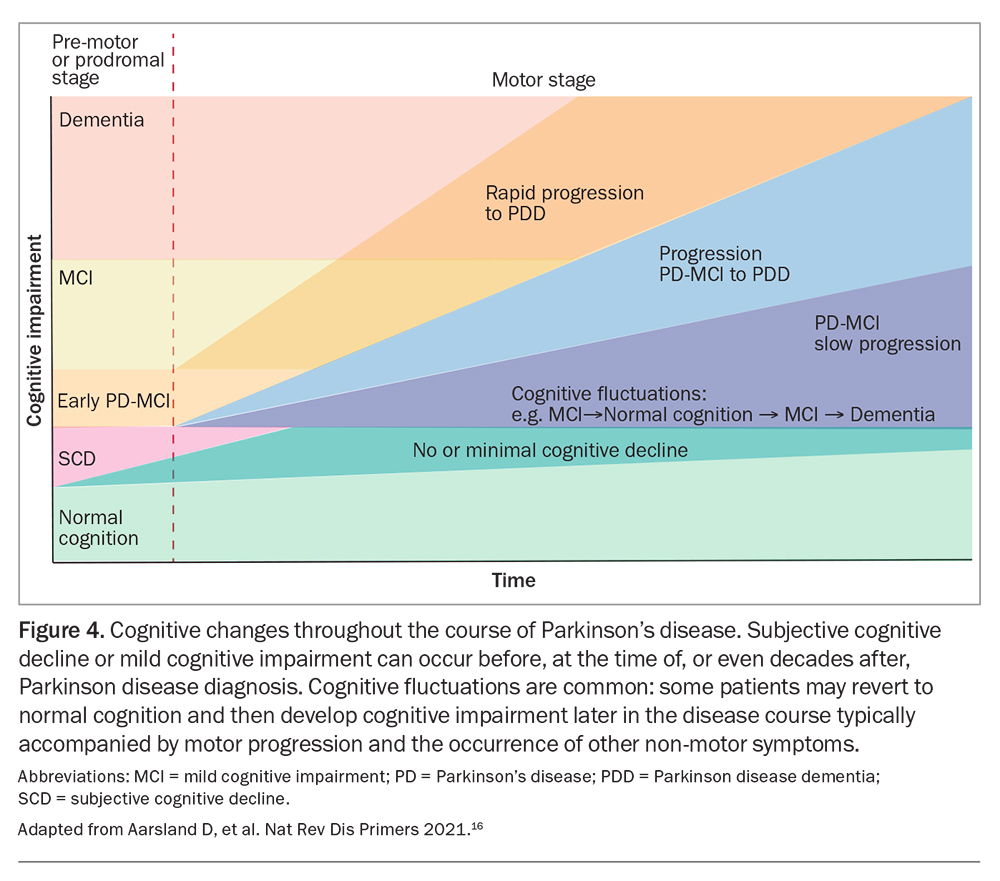
Although present in early disease, cognitive impairment impacts more significantly on patients with advancing age and longer disease duration (Figure 4).2,16 Mental and physical stimulation through activities, social engagement and exercise independently improve cognitive performance. Management of other risk factors such as hypertension, hypercholesterolaemia and diabetes is also protective against cognitive decline. Consideration should be given to withdrawal of agents with anticholinergic effects, which can exacerbate cognitive symptoms. Cholinesterase inhibition with rivastigmine has been shown to benefit patients with Parkinson’s disease and dementia, but studies with donepezil, galantamine and memantine have not achieved study endpoints. Unfortunately, these drugs are only PBS subsidised for patients with Alzheimer’s disease.
{kind=link}
Conclusion
Parkinson’s disease is a multisystemic condition with profound effects on movement, mood, sleep and autonomic function. Advanced disease requires a multifaceted approach to management, tailored to the individual patient, including lifestyle, pharmacological and sometimes neurosurgical interventions. Significant input from allied health professional at every stage of management provides the gold standard for assessment and subsequent optimal management of the condition. MT
COMPETING INTERESTS: None.