Rare diseases – new approaches to diagnosis and care

Two million people in Australia live with a rare disease and face common challenges of diagnostic delay, lack of clinical knowledge and treatment and fragmented care, as well as significant psychosocial impacts. Caring for patients with rare diseases and their families requires innovative collaborative approaches across institutional, geographical and system boundaries. New resources and toolkits that prioritise improved diagnosis, care and support are available to help GPs provide excellence in rare disease care for patients and their families.
In 2020, the Australian Government launched the first nationally co-ordinated policy approach to address rare diseases in Australia: the National Strategic Action Plan for Rare Diseases.1 The plan recognises common challenges facing those living with rare diseases and priorities to improve diagnosis, care and support. This article highlights these common challenges and new approaches and resources that have been launched to help doctors in Australia address these priorities. As GPs are the healthcare professionals most often responsible for identifying people with a likely rare disease and co-ordinating whole of life interdisciplinary care and support for patients and their families, many of these resources have been codesigned with their input.2 Developments in rare disease care across other areas of medical care and research were highlighted in a recent review article and are not addressed fully here.3
Why think about a new approach to rare diseases?
Rare diseases impact a relatively small number of individuals, with a prevalence of less than five in 10,000, and about 80% are genetic, such as cystic fibrosis and Noonan syndrome.3 Non- genetic rare diseases include rare autoimmune conditions such as scleroderma, rare oncological conditions such as mesothelioma and rare infections such as Barmah Forest virus.
Rapid advances in diagnostic testing, such as genomic sequencing, have allowed the continued increase in the diagnosis of individuals with a rare disease, with over 7000 individual rare diseases recognised.4 Despite their individual rarity, rare diseases are now recognised to be collectively common and estimated to affect about two million people across Australia.4 A full-time equivalent GP therefore has 60 to 70 patients with a rare disease in their practice.
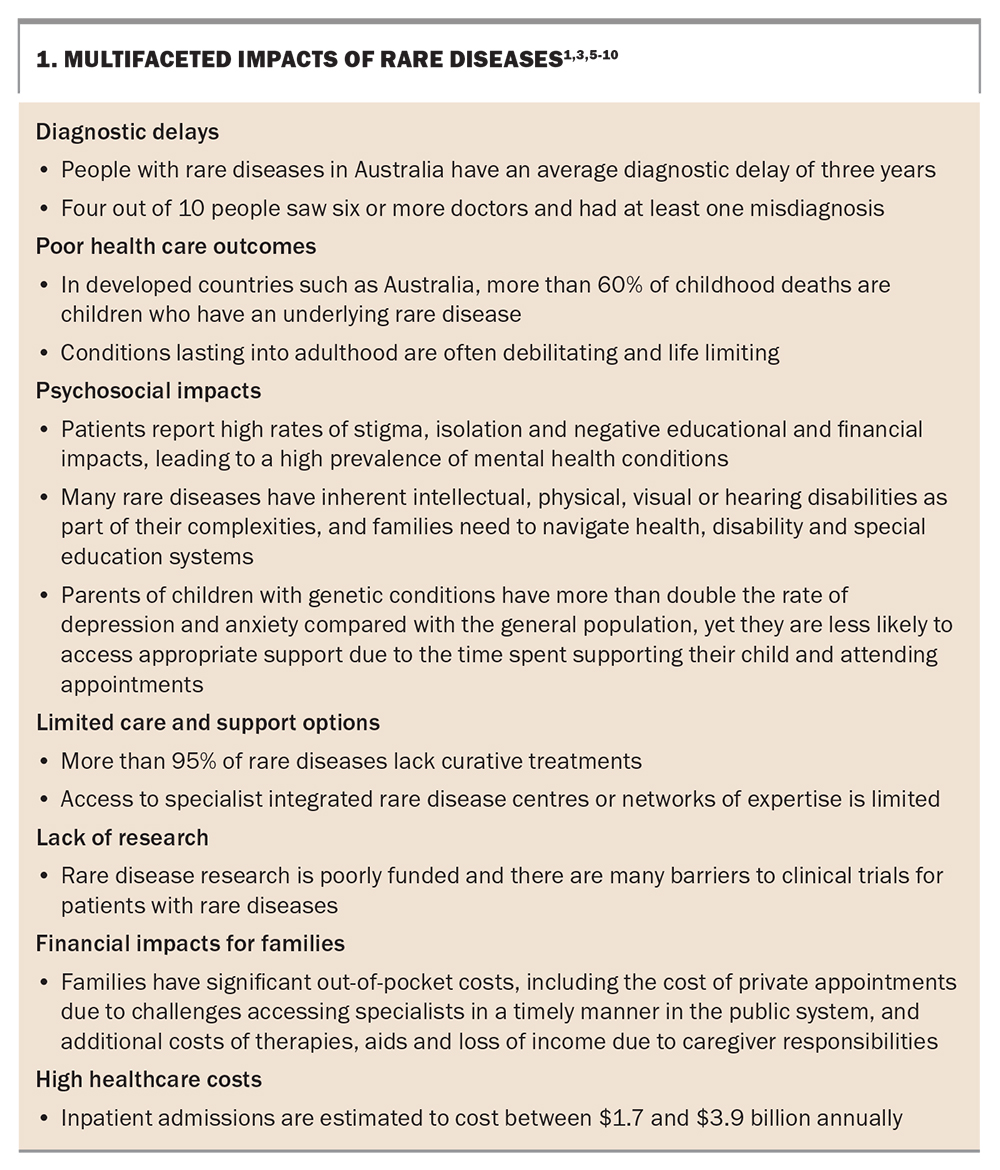
Most rare diseases (82%) have onset in childhood, are chronic, have no known treatment and continue throughout the lifespan. Patients with a rare disease and their families face distinct, often more severe and complex challenges with multifaceted impacts, compared with those with more common chronic conditions, such as diabetes, because of their relative rarity and often complex multiorgan involvement (Box 1).1,3,5-10 These challenges were recognised in Australia’s 2020 National Strategic Action Plan for Rare Diseases, which explicitly called for innovative models of care for rare diseases to tackle these critical challenges.1 This need was echoed globally at the end of 2021 by the first-ever United Nations resolution on Addressing the Challenges of Persons Living with a Rare Disease and their Families.11
{kind=link}
Australia’s distinct geography and population demographics have resulted in dispersed, fragmented research expertise that is often geographically distant from a patient’s usual care team.3 Access to rare disease diagnoses and expert care is particularly challenging for people living in rural, regional and remote Australia, those who are from Aboriginal and Torres Strait Islander and culturally and linguistically diverse communities, and those who have low health literacy and socioeconomic status.1
People living with rare diseases and their carers in Australia, as in other countries, have expressed dissatisfaction with their health care and support.5,6,12 Moreover, healthcare professionals have reported that challenges in accessing appropriate specialist services and lack of management guidelines and appropriate healthcare infrastructure, along with difficulties appropriately coding rare diseases and paucity of sustainable rare disease registries, hinder their ability to provide high-quality, timely and integrated care.2,3
Tools to improve awareness of rare disease
Diagnostic delay is a major challenge of rare diseases, with families waiting an average of three years for a diagnosis, if one is ever made; four out of 10 people with a rare disease reported seeing more than six doctors and had at least one misdiagnosis before their rare disease was recognised and diagnosed.6 This long diagnostic odyssey has significant impacts the mental health and wellbeing of patients and their families, resulting in uncertainty, stigma and frustration with healthcare professionals and the community at not being believed that a ‘real’ medical condition exists.13
The ‘Family GENES’ mnemonic
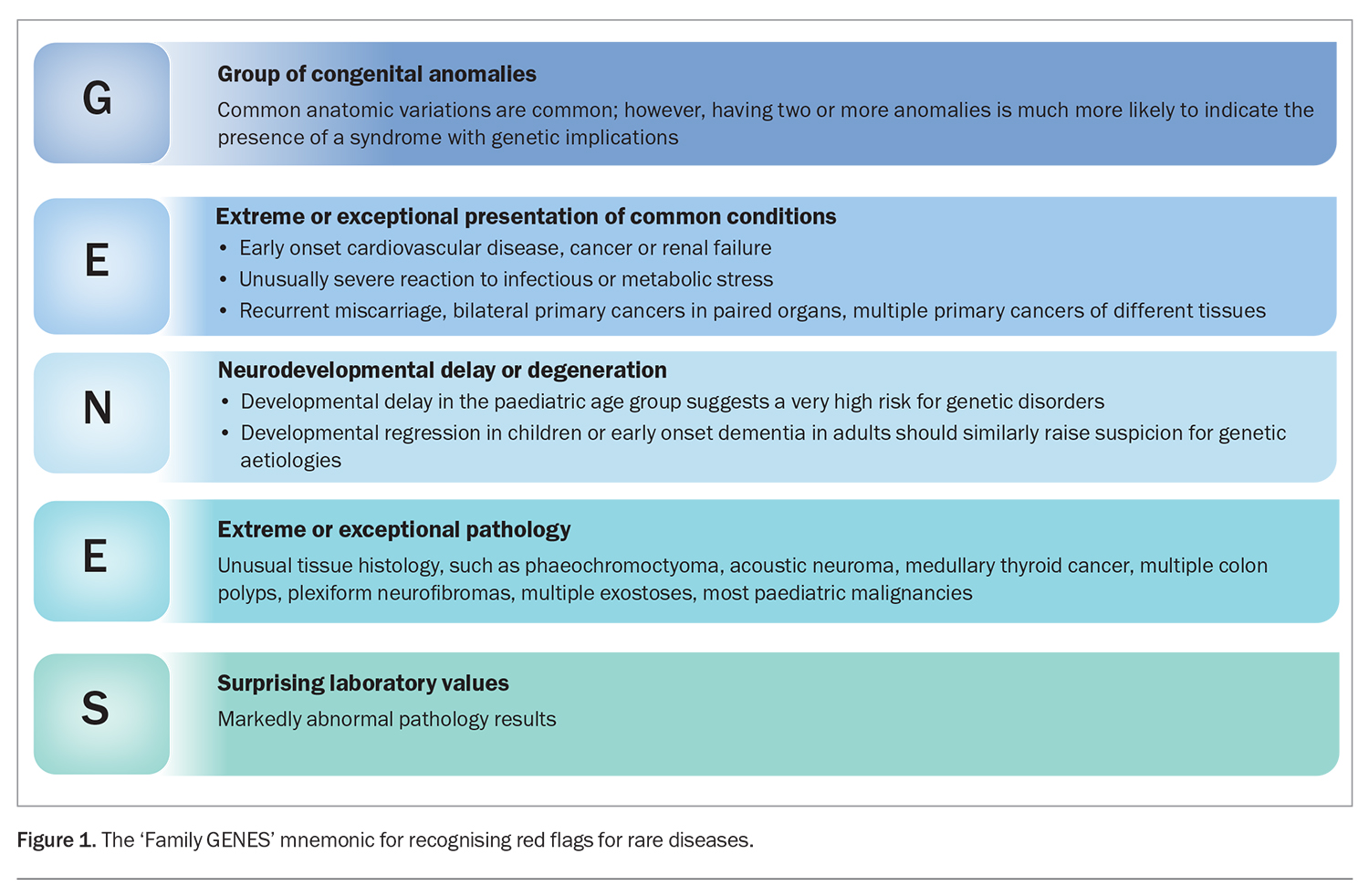
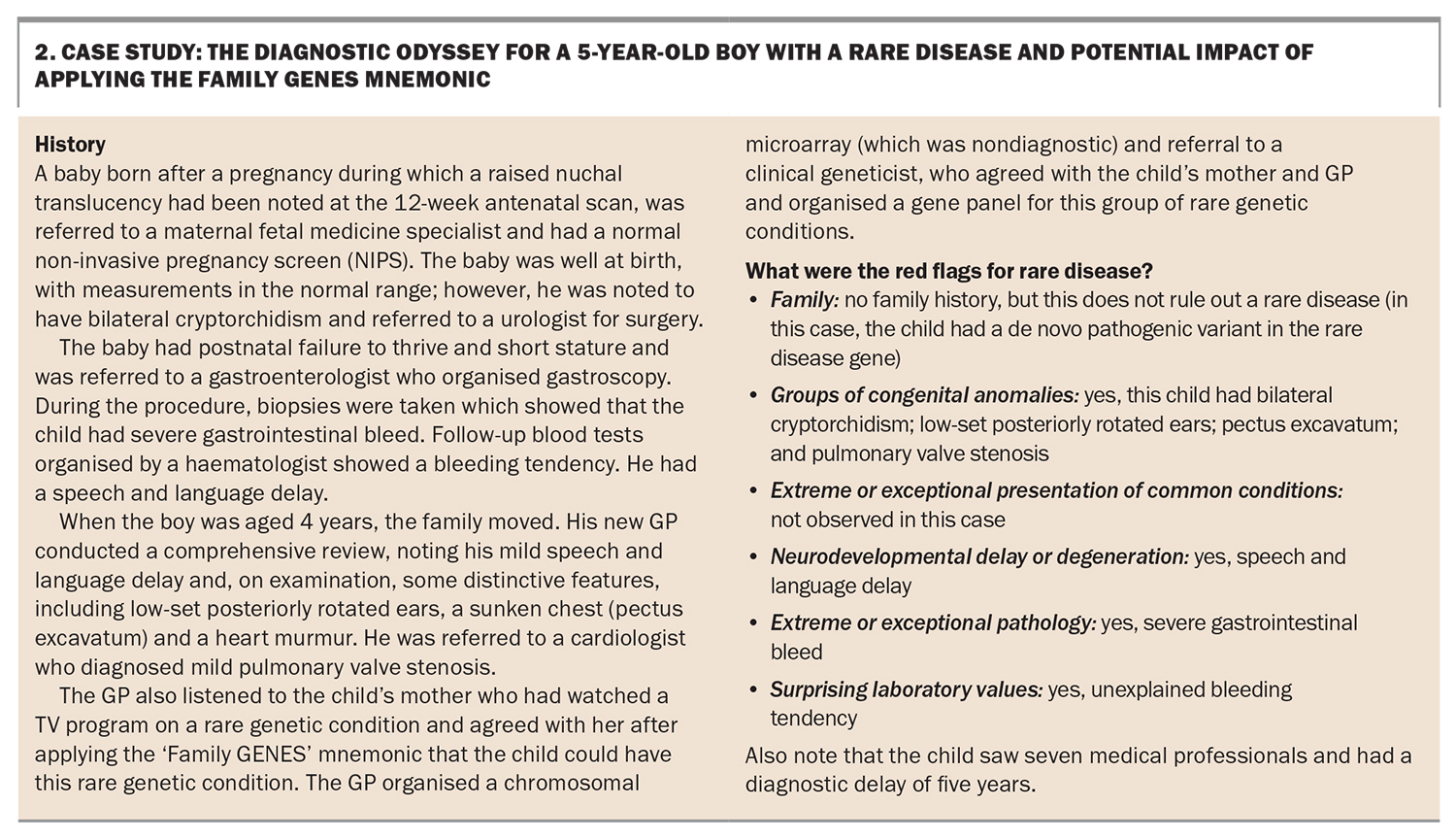
A simple mnemonic ‘Family GENES’ was developed by a US Genetics in Primary Care Faculty Development Initiative to help alert clinicians that their patient might have a rare disease (Figure 1).14 Box 2 outlines a case scenario in which application of this mnemonic may have shortened the diagnostic odyssey for the patient and their family.
{kind=link}
{kind=link}
The Family GENES tool does not identify what rare disease an individual has, rather it helps signpost that a referral to a diagnostic centre, such as a clinical genetics service, or a centre of expertise in managing the most significant patient symptoms should be considered. For example, six-month-old diamniotic twins with persistent respiratory distress, cough and failure to thrive may be referred to a paediatric respiratory physician with expertise in childhood interstitial lung diseases.
Online search engines
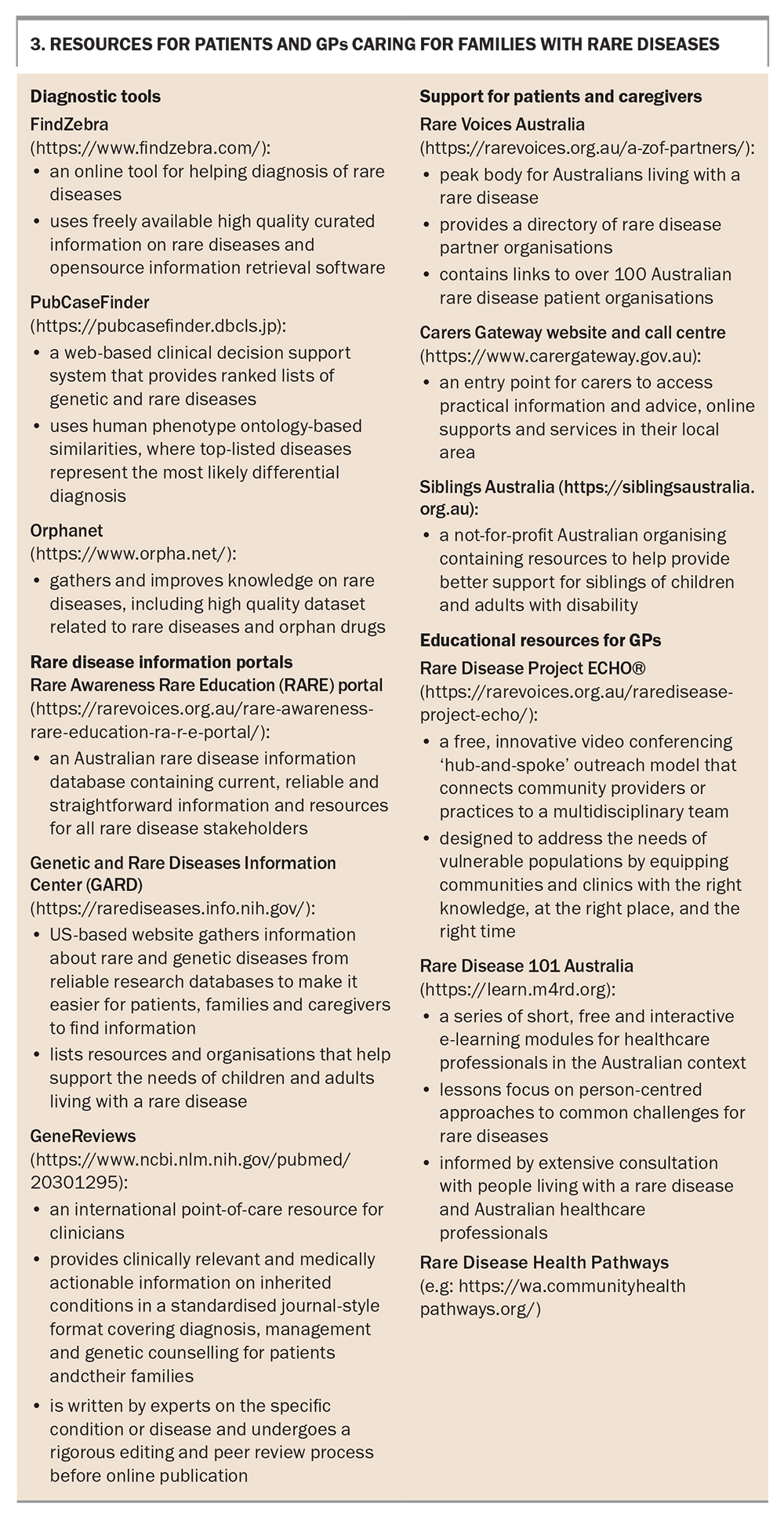
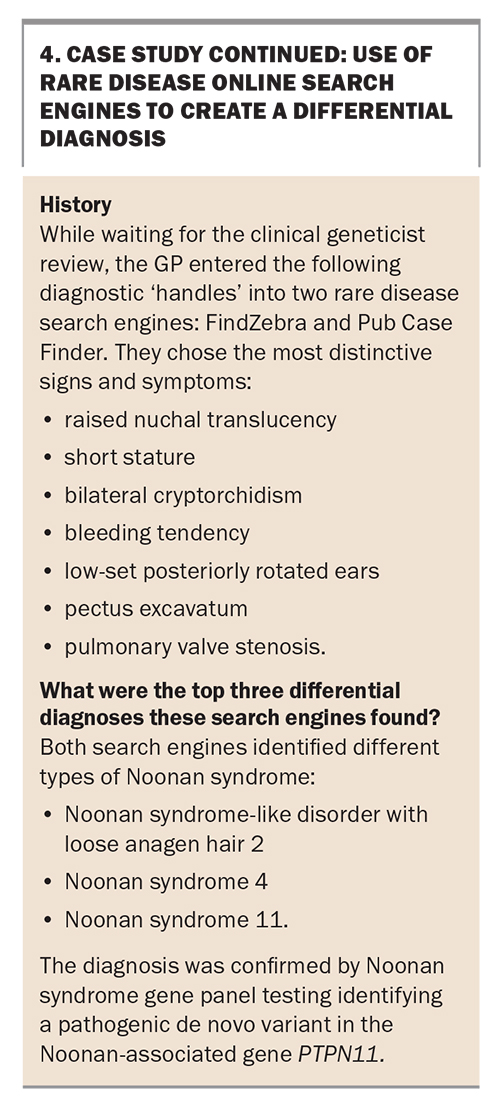
Because of national workforce shortages, such as in clinical geneticists and metabolic experts, and lack of rare disease centres or a network of expertise, waiting times for such diagnostic expert review can be frustratingly long.3 Therefore, GPs may consider one of the open access tools to help construct a differential diagnosis.15 Traditional search engines, such as PubMed and Online Mendelian Inheritance in Man (OMIM), are well known; however, a growing number of search engines are optimised to help diagnose rare diseases.16,17 Clinicians, or indeed patients or carers, can enter key phenotype information, and these search engines return potential underlying diseases and genes involved. Examples of these intuitive tools are shown in the Box 3. They include FindZebra and PubCaseFinder. A worked example of their use is shown in Box 4.16,17
{kind=link}
{kind=link}
These tools can assist a clinician only when they have recognised and distilled the key signs and symptoms after carefully listening to the patient and their family, taking a thorough clinical and family history spanning three generations, and performing a thorough examination. Many families with a rare disease only receive a diagnosis once a clinician takes the time to perform such an extensive diagnostic review, which often requires longer appointments to allow the key diagnostic ‘handles’ to emerge.13
Diagnostic pathways for rare diseases
Increased accessibility via dedicated Medicare item numbers for unbiased genomic tests, such as chromosomal microarray, exome and whole genome sequencing, is increasing the number of people diagnosed with a rare genetic condition.4,18 For example, in the October 2022 issue of Medicine Today, we discussed how the application of unbiased exome or genomic sequencing can diagnose over 50% of children with severe early onset epilepsy accompanied by developmental delay, a constellation of symptoms only recently recognised to have a potential genetic aetiology.19
However, for many individuals suspected of having a monogenic condition, a diagnosis cannot be reached using available testing. New undiagnosed disease programs, such as the Undiagnosed Diseases Network of Australia and the Undiagnosed Diseases Network International, offer opportunities for clinicians to enrol patients’ families in cutting-edge clinical research that applies genomic reanalysis, international case ‘matchmaking’ and new frontier multiomic tools, such as RNA sequencing, to further boost diagnostic yields.18,20 Artificial intelligence is also helping with diagnoses; for example, the online resource FaceMatch (https://facematch.org.au/home) uses artificial intelligence-assisted face-matching technology to help parents and clinicians of children who have distinctive facial features, yet remain undiagnosed, find a specific rare disease diagnosis.21
After a rare disease diagnosis
An aetiological diagnosis ends a family’s diagnostic odyssey, provides accurate reproductive counselling and, potentially, reduces stigma associated with being disbelieved to have a ‘real’ condition. A diagnosis may also alleviate misattributed guilt, particularly from parents who thought the condition could have been caused by something they did or did not do, for example during pregnancy.22 However, a rare disease is often, by its very nature, one that their GP and specialists have never heard of, and for which no management guidelines, optimal therapies or easily accessible lay information exists; over 95% of rare diseases currently lack a prognosis-altering therapy.3 Thus, a rare disease diagnosis frequently leads to more uncertainties.23
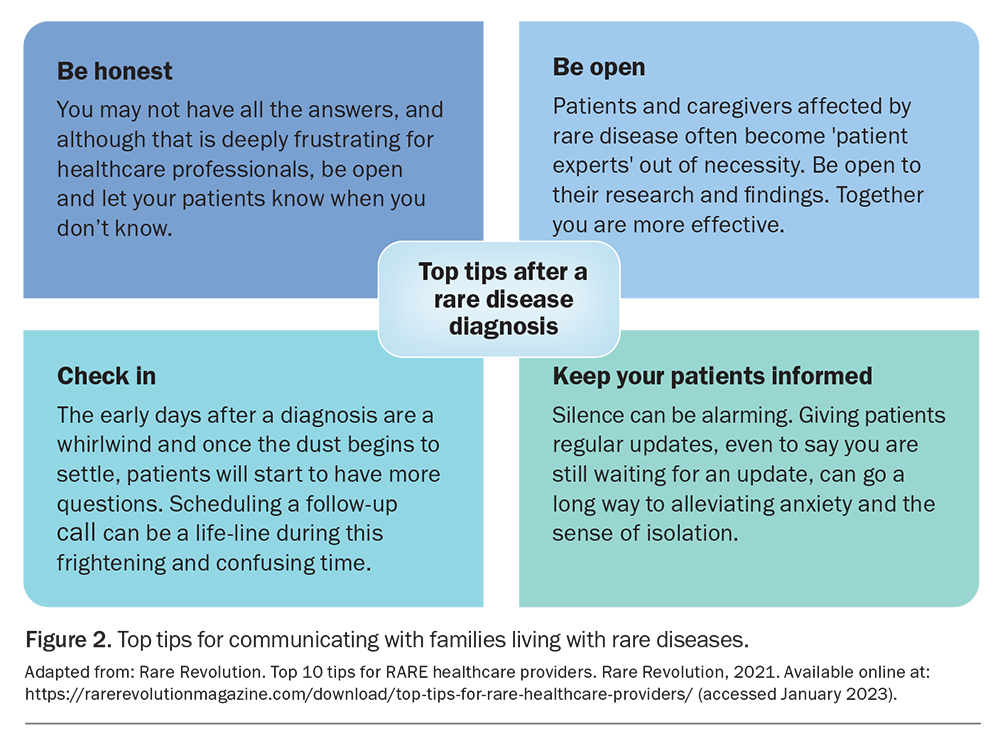
Given the well-recognised multifaceted impacts of rare diseases on patients and their families and carers (Box 1), the GP’s role in providing support, guidance and open communication is foundational.9 In our experience, families living with a rare disease prefer that their doctor (Figure 2):24
{kind=link}
- acknowledge honestly unfamiliarity with the rare diagnosis
- agree to partner with the patient and their family and be open to their patient’s own research
- help signpost reliable curated information resources (Box 3)
- continue to regularly ‘check in’ on how the family is doing and proactively support their mental health and wellbeing
- advocate for appropriate financial and disability support.
A proactive and hopeful approach is also justified, as rare disease translational research is constantly progressing. New therapies that do not just address symptoms but target the underlying pathophysiology are increasingly being developed, trialled and becoming available. For example, advances in gene-based therapies for spinal muscular atrophy and targeted therapies for cystic fibrosis have improved outcomes and prognosis for children with these rare conditions, allowing them to survive and thrive.25,26
Often, rare disease patient advocacy groups are lifelines for families with a rare disease and their clinical teams: they help connect families who are on a similar journey; direct clinicians and families to reliable, up-to-date clinical information and guidelines; and alert them to centres of clinical expertise, new research opportunities and availability of advanced therapeutics.27 Thus, in the internet age, reliable sources of information (such as those listed in Box 3) is more helpful than the old adage ‘don't google this’ to patients, families and clinicians alike. Rare Voices Australia, the national peak body for rare diseases, is launching the Rare Awareness Rare Education (RARE) portal, which contains current, reliable and straightforward information and resources for all rare disease stakeholders, customised to the Australian context and informed by robust extensive multistakeholder consultation.
New educational resources for rare disease care in Australia
The national Rare Disease Awareness, Education, Support and Training (RArEST) project is currently conducting a learning needs assessment for Australian healthcare professionals. So far, fewer than 5% of surveyed clinicians strongly agree that the healthcare systems in which they work make it easy for them to support rare disease patients, despite over 80% agreeing that specific rare disease care was an important part of their role. To enable them to provide more streamlined and integrated care and support to families with a rare disease, clinicians have prioritised the need for:
- easily accessible information and resources
- clear guidelines for the identification and management of rare diseases
- changes in healthcare infrastructure to enable them to provide more streamlined and integrated care and support to families with a rare disease.
To meet these challenges the RArEST project has codesigned, with people living with rare disease and clinicians in Australia, free educational supports and resources including:
- a community of clinical learning practice
- the Rare Disease Project ECHO, which aims to address the needs of vulnerable populations by connecting community providers and practices to shared knowledge and relevant multidisciplinary expertise
- Rare Disease 101 Australia, a flexible digital learning module that includes nine lessons covering key topics for health practitioners in the Australian context, including rare disease diagnostic tools, genomics, how to effectively partner with patient advocacy groups and keep up-to-date with rare disease research and novel therapies.
More information about these new Australian rare disease resources is provided in Box 3 and on the RArEST project website (https://rarevoices.org.au/rarest-project/).
Conclusion
Australia’s National Strategic Action Plan for Rare Diseases highlights priorities that must be addressed to improve outcomes for the two million Australians living with a rare disease. This need is echoed by the global ‘rare disease movement’, which succeeded in the ratification of the 2020 United Nations Resolution on Persons Living with a Rare Disease. Advances in rare disease diagnostic tools and genomics have the potential to significantly help GPs and other healthcare professionals access rare disease diagnoses. A range of new clinical educational tools and resources are available to support clinicians in partnering with their patients with a rare disease to ensure person-centred, whole-of-life support and care. Ongoing developments in rare disease research and advanced therapeutics continue to provide hope for patients with rare diseases and their families. MT
COMPETING INTERESTS: Professor Baynam: None. Dr Palmer, Professor Zurynski and Professor Jaffe have received government grants for the RArEST Project; and are Members of the Scientific and Medical Advisory Committee for Rare Voices Australia. Ms Millis has received government grants for the RArEST and RARE projects; and project funding and membership to support RVA projects from the Round Table of Companies (https://rarevoices.org.au/round-table-of-companies/). Professor Farrar has received government grants for the RArEST project and honoraria from Biogen, Novartis and Roche for educational presentations and sitting on scientific advisory boards; and is a Member of Scientific and Medical Advisory Committee for Childhood Dementia Initiative and Medical Director for Muscular Dystrophy New South Wales.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.