Genomics: what it means for patients and GPs

Genetic disorders
Genetic testing
Genomics is an important emerging field in medicine that will have increasing relevance in general practice. This article outlines the current utility of genomics and provides information to enable discussion about the application of genomics.
- Over the past decade genomic testing has become more accessible and affordable with results available much sooner.
- Genomic tests, particularly whole exome and whole genome sequencing, are now increasingly used to diagnose patients with Mendelian genetic diseases including syndromal intellectual disability, cardiac disease and cancer.
- Genomic tests are more recently being used in preventive health. This includes pharmacogenomics testing and testing of healthy individuals for genes that are rare but significantly increase disease risk.
- Patients’ genomic data will become more accessible in the future and is set to play an increasing role in guiding patient care.
The Human Genome Project, completed in 2003, was a combined global effort to map the human genome as a reference source.1 Tools developed during this project provided the catalyst for the subsequent significant advances in genomic technology to enable rapid and cheaper genome sequencing and improved interpretation of genomic data. The technology is often referred to as next generation sequencing (NGS) or massively parallel sequencing (MPS) and the term genomics refers to the use of this technology to sequence either the entire genome – whole genome sequencing (WGS) – or all the genes in the genome – whole exome sequencing (WES).
The advantage of genomic technologies over more traditional genetic testing modalities is that WES and WGS allow for a broader diagnostic search for the underlying genetic cause in an individual suspected or known to have a genetic disease. Over the past decade, genomic sequencing has gone from being a research-based tool to a testing option that is being used widely in clinical practice.2
Types of testing
Many different genetic tests are available and used in patient care for purposes ranging from diagnosis of rare genetic conditions to preconception carrier screening. Although Medicare rebates are available for some genetic tests (such as those for haemochromatosis and Fragile X syndrome), there is currently no Medicare rebate for many others, including genomic testing. The cost of the tests varies depending on which laboratory is offering the test and is largely determined by the technology used, the number of genes covered, the speed of the result and the country in which the laboratory is based. Patients seen through public clinical genetics services when offered testing usually have no out-of-pocket costs, which is an important consideration as some genetic test costs are high.
Single-gene and multi-gene panel tests
There is a wide range of genetic tests available, including single gene tests for conditions that have a single gene basis such as cystic fibrosis and tests for panels (groups) of genes known to be associated with specific genetic diseases or organ pathology that are genetically heterogeneous (i.e. could be caused by one of many genes). Laboratories are increasingly moving to gene panel testing via NGS to increase the number of genes tested and reduce costs. Gene panels commonly used include those for cardiac diseases such as cardiomyopathy, ocular disorders such as retinitis pigmentosa and neurological disorders such as epilepsy.
Whole exome and whole genome sequencing
The major difference between WES and WGS is that WES is designed to capture only the exome, the protein-coding portion of the gene, and WGS produces data across the entire genome. Although the exome comprises less than 1.5% of the total genome, it carries most of the genetic variation known to cause disease (pathogenic variant).3 WGS produces data on noncoding regions that have recently been shown to have important roles such as gene expression;4 however, variation in these regions remains difficult to interpret for clinical use. Although a specific set of genes can be analysed from WES or WGS, often these technologies are used for a broad analysis of all known human disease genes and variation in these are linked to the patient’s clinical features.
Although WGS is a more expensive test than WES, it provides higher diagnostic return than WES. This is partly because of more consistent sequencing coverage of genes, improved detection of copy number variation (where sections of the genome are duplicated or deleted)5 and sequencing of the mitochondrial genome.
Testing practicalities
GPs generally counsel patients and order some genetic tests such as for haemochromatosis. They may be increasingly involved in preconception carrier screening for couples planning a pregnancy with or without a known personal or family history of genetic disease.
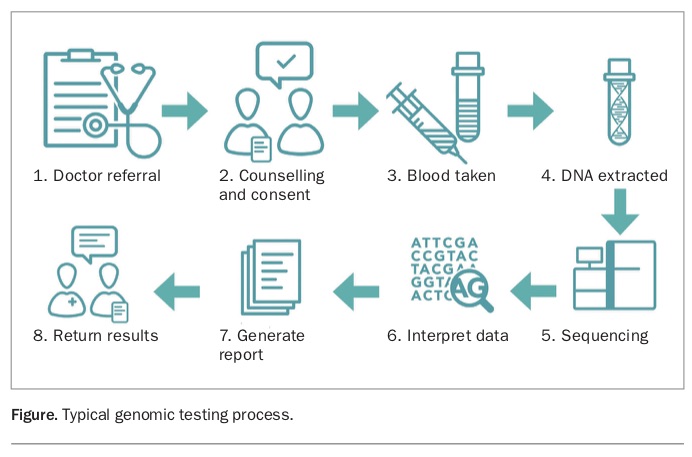
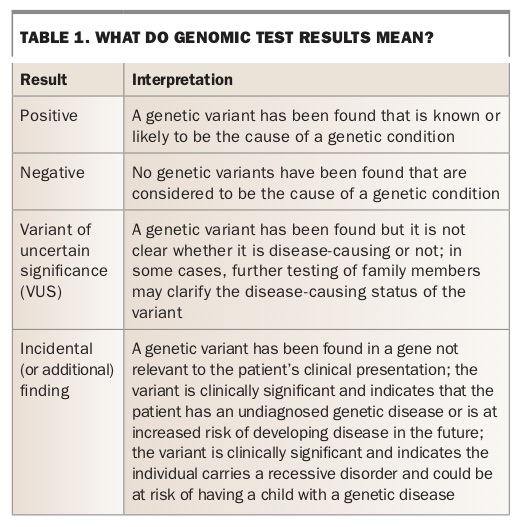
However, patients with complex or rare conditions who may benefit from genomic testing are usually referred to a specialist genetics clinic or a relevant specialist for further assessment. The typical process of genomic testing is outlined in the Figure and how to interpret the results is listed in Table 1.
{kind=link}
{kind=link}
Applications of genomics
Genomic testing is routinely used to aid the diagnosis of complex, rare and suspected genetic diseases. Its greatest use to date has been in patients in whom it has not been possible to make a diagnosis based on their clinical presentation or when there are several genes that could be causative.6 The key to making a diagnosis is to be able to make the link between the patient’s clinical features, their phenotype, and the genetic variation, genotype. This clinical interpretation of genomic data is challenging and requires unique skill sets to link the patient phenotype to the correct gene variant(s) responsible for disease in that patient from a large list of possible variants.
Australian research suggests that children who are likely to have a rare undiagnosed condition should be referred early to clinical genetic specialists for WES, because it has been shown to be a cost-effective option compared with traditional diagnostic pathways.7,8
Pharmacogenomic testing examines common genetic variation that influences an individual’s drug metabolism and is increasingly being utilised. An individual who metabolises a particular drug rapidly may clear the drug too quickly, rendering it ineffective. Conversely, those who metabolise the drug too slowly may experience toxic effects. Prescribed drugs that are often included in pharmacogenomics testing include analgesics, antidepressants, anticoagulants and statins. If pharmacogenomic test results are readily accessible as part of a patient’s electronic health record, they will prove a useful tool to guide prescribing decisions and reduce adverse events.9
One of the newest applications of genomic testing is for healthy individuals to have their genome sequenced and analysed to assess if their risk of developing certain genetic diseases is increased. It is possible to assess whether an individual carries a gene variant that can predispose them to rare heritable genetic disorders such as cardiomyopathy or a familial cancer syndrome (e.g. BRCA1 or BRCA2). Interpreting such a variant without a corresponding disease or family history can be challenging so a high level of confidence that the variant is disease-causing is needed for reporting. Although the proportion of individuals with a positive finding from this type of personal genomic testing is relatively low, knowing such information can enable them to manage the increased risk, including undertaking more regular screening or risk-reduction strategies such as medication or lifestyle changes.10
The RACGP recently released guidelines on the use of personal genomic testing that stated the clinical utility of such testing was variable.11 It recommended that patients who wish to pursue personal genomic testing should opt for a full-service provider that includes the need for referral by a GP, test interpretation and genetic counselling support.
Implications of genomics in primary practice
When a patient discovers through a genomic test that they or a family member has a genetic condition, this can lead to a number of outcomes. They may require additional screening for particular conditions for which they are at increased risk, or they may have a new understanding of inheritance patterns that has implications for family planning and other family members. GPs have an important role in assisting patients with medical and psychosocial support and providing referrals to appropriate specialists.
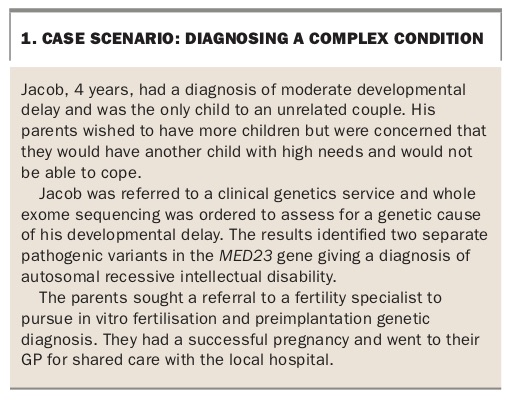
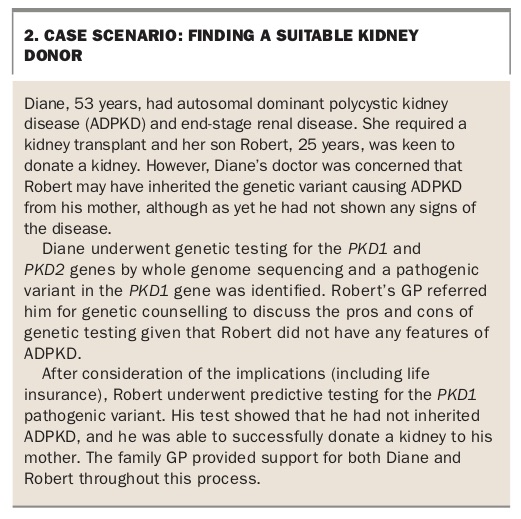
The case scenarios in Box 1, Box 2, Box 3, Box 4, Box 5 and Box 6 highlight different ways in which genomics can impact primary care practice.11,12 Some GP resources are provided in Box 7.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Genetic counselling and patient considerations
There are several factors that patients should consider before having a genomic test. Genetic counselling should be an integral part of the testing process and can be provided by a genetic counsellor, clinical geneticist or experienced medical specialist (Box 8). The role of genetic counselling involves ensuring the patient understands the test they are having and what information it can and cannot provide, as well as explaining the practical information about the testing process.
{kind=link}
Genetic counselling can be provided face-to-face or through telehealth (telephone or online counselling). The aim is to help patients to consider what their motivation is for having the test, what they are hoping the test will achieve, and how they will adapt to the results, whether they are positive, negative or inconclusive. Patients also need to be aware that their test findings may have implications for their family members, including their siblings and children.
If patients are undergoing WES or WGS, there is a small possibility the testing will reveal incidental findings – a genetic variant found in a gene not relevant to the patient’s clinical presentation. It is important that this possibility is discussed as part of the testing consent process and that the patient is clear about what information they want returned.
Although genetic results do not affect private health insurance premiums, they can have implications for risk-rated insurance policies such as life insurance, disability insurance and income protection insurance (Box 9).13 Genomic data are a lifetime resource that will likely form an integral part of patients’ medical records in the future. Given the value of this data, it is also important that patients and their clinicians consider factors such as whether the testing laboratory is clinically accredited and what policies it has regarding data security, privacy and access and any possible future uses of their data.
{kind=link}
How will genomics change the way doctors practise in the future?
One of the first areas where GPs are likely to feel the impact of a shift towards greater clinical use of genomic data is in the area of reproductive carrier screening. In this year’s Federal Budget, the Government announced a $500 million, 10-year Australian Genomics Health Futures Mission,14 which will begin with a $20 million preconception screening trial for birth disorders including spinal muscular atrophy, Fragile X syndrome and cystic fibrosis.
Genomic sequencing, unlike traditional pathology tests, can provide ongoing personal health utility. This can be accessed through reanalysis of the data in response to a new health issue or to search again for a genetic disease cause from a previously negative test result with the emergence of new genetic knowledge. In the future, if these data can be fully integrated into our healthcare systems and become available at the point of care, it will enable precision medicine with GPs and other clinicians able to personalise healthcare for individual patients.
Conclusion
Genomic testing is increasingly being used in patient care to diagnose, screen for and assess risk of inherited conditions and diseases. GPs will increasingly have access to patients’ genomic data to help guide their clinical decision-making. MT
References
LifeInsurance/Report (accessed July 2018).
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.