Importance and challenges of vaccination in older people


Immunisation
Infectious diseases
Infectious diseases contribute significantly to morbidity, ongoing functional decline and mortality in older people. Several of these diseases are preventable by vaccination, but vaccine coverage is suboptimal for all of these. New approaches are required to improve vaccine coverage among people aged 65 years and over.
- A decline in immune function with ageing increases the impact of infectious diseases in older people.
- This immunosenescence also decreases the effectiveness of vaccines in older people.
- Older people should be provided with pneumococcal, herpes zoster and booster pertussis vaccines as well as annual influenza vaccine.
- Poor data on vaccine coverage and burden of disease have hampered efforts to increase vaccine coverage; some patients and clinicians are sceptical about the need for vaccines and their effectiveness. Better monitoring might help combat this.
- A new approach to advocacy involving a broader partnership base is required, to educate the public and deliver vaccines.
- Vaccines recommended on a scientific basis should be funded under the National Immunisation Program.
Older people undergo an age-related decline in immune responses resulting in greater susceptibility to infection and reduced responses to vaccination.1 This decline in immune function, termed immunosenescence, affects both innate and adaptive immune systems. Essential features of immunosenescence include reduced natural killer cell cytotoxicity on a per cell basis, and decreased pools of naive T and B cells. There is an accumulation of late-differentiated effector T cells, commonly associated with cytomegalovirus infection, which contributes to a decline in the capacity of the adaptive immune system to respond to novel antigens. The reduced functional capacity of T cells is the main effect of the ageing process.2 Immunosenescence is a major contributory factor to the increased frequency of morbidity and mortality among older people and the reduction in vaccine responsiveness in this age group, especially frail patients.
Infectious diseases are significant in older people not just because of their increased severity (e.g. more than 90% of influenza deaths are in people aged over 65 years) but also because of their impact on functional capacity after the illness. Data show that hospitalisation for influenza is highly likely to lead to ‘catastrophic disability’, defined as a loss of three levels of capacity for activities of daily living.3 Typically, older people who are independent at home and are hospitalised with influenza need assistance with care on discharge.
Similar data exist for people with shingles. A French study showed ongoing deficits in physical, social and psychological functioning after older people developed postherpetic neuralgia.4
Vaccines available for older people
Although not all recommended vaccines are funded for older people in Australia, GPs should ensure that every 65-year-old patient receives:
- an enhanced influenza vaccine and ongoing annual vaccination
- first-dose 23-valent polysaccharide pneumococcal vaccine, with boosters if required
- herpes zoster vaccine
- an acellular pertussis vaccine booster if this has not been given in the previous 10 years.
Vaccine coverage in older people
In Australia, accurate data on vaccine coverage levels are available for the paediatric vaccination program but not for vaccination coverage of older people. The most recent national survey of vaccine coverage in older adults was conducted in 2009. Estimates derived from more recent ad-hoc surveys suggest that:
- about 75 to 80% of older people receive influenza vaccines each year
- about 50% have received a pneumococcal vaccine
- about 25 to 30% have received a herpes zoster vaccine (albeit more in the 70 to 79 years age group)
- fewer than 10% have received a pertussis booster in the past 10 years.
The recent expansion of the Australian Childhood Immunisation Register (ACIR) into a whole-of-life Australian Immunisation Register (AIR) has the potential to improve data on older people over time. However, this will depend on the support of GPs to input data as they vaccinate older people. It will also require data entry at other sites where vaccines are provided, such as pharmacies. Further, the absence of a mechanism to input historical data will reduce the accuracy of coverage data for all vaccines other than the annual influenza vaccine for many years.
Burden of vaccine-preventable disease in older people
Similarly, accurate data on vaccine-preventable disease rates in older people are not available. Many older people with influenza are not tested or notified to public health authorities; presenting symptoms may be a worsening of a chronic condition, or confusion alone, and more than half of patients have no fever.5 Many patients with shingles are diagnosed clinically and are not investigated. Most patients with pertussis present with a chronic cough and do not have a swab taken. About 20% of patients presenting with a chronic cough of more than two weeks’ duration have pertussis.6 Community-acquired pneumonia is rarely confirmed as being due to Streptococcus pneumoniae (pneumococcus).
The failure to describe adequately the morbidity and mortality associated with vaccine-preventable diseases in older people is a major impediment to improving vaccine uptake. Lack of awareness of the significance of a problem reduces the likelihood of preventive action. Despite the high percentage of older people developing shingles (with 50% of 85-year-olds having had the disease7) and the seriousness of postherpetic neuralgia, a community survey conducted by a vaccine manufacturer found that only 4% of older people were concerned about the disease. The lack of understanding of the significance of these illnesses extends to healthcare providers, with few understanding the seriousness of pertussis infection for older people themselves, not only for their newborn grandchildren.
Improving vaccine uptake in older people
Some pre-conditions and requirements for improving vaccine uptake in older people are outlined in the Table.
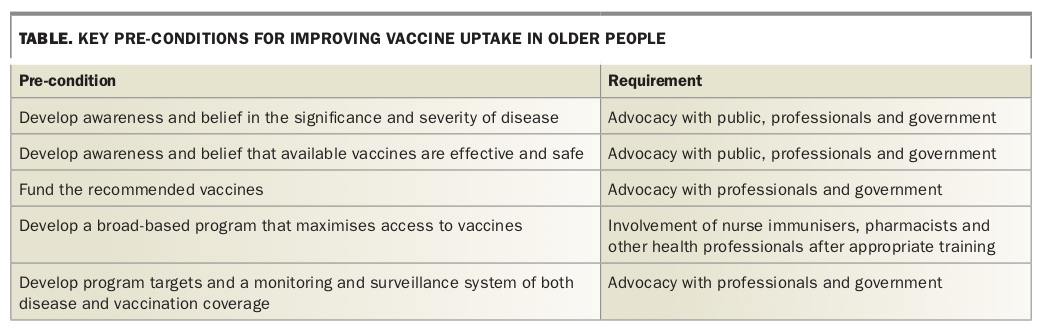{kind=link}
Better understanding of disease burden and vaccine benefits
Developing a better understanding of the balance of risks versus benefits of vaccines in older people involves engaging not just health practitioners but also the public, media and governments. The initial step involves providing strong evidence about the burden of vaccine-preventable disease, put simply, and incorporating health literacy development.8 Having available product champions from among target groups as well as skilled media performers is important once messages are ready, as is engaging nontraditional partners in message development, such as groups representing aged people or people living with chronic diseases.
Although providing education to GPs that emphasises whole-of-life vaccination and vaccination of older people is necessary, opportunities also exist to involve nurse immunisers, immunisation alliances, pharmacists and key nongovernment organisations such as COTA (formerly Council on the Ageing), Diabetes Australia and other organisations representing target groups. Despite the lack of support for these ‘nontraditional’ sources of vaccination in some sectors, their scope is increasing, and they should be involved in messaging to ensure consistent activity.9 Although many older people still use traditional media, an increasing proportion access the internet, and enhanced promotional activity on social media might also improve uptake.
Largely due to immunosenescence, many vaccines are only partly effective in older people, leading to a reduced commitment to their use by both the public and health professionals. Modified messages about vaccination are required to address this. For example, although some older people develop influenza despite being vaccinated, their illness will be attenuated, and they will be less likely to be hospitalised.10 Also, new enhanced influenza vaccines produce a better response than traditional inactivated influenza vaccines. GPs need to convey the dangers of not being vaccinated.
Systems approaches in general practice
GPs also need to develop strategies to increase coverage within their practices. These strategies should include a systems approach to identify target populations and engage with them. For example, use of electronic records and desktop software to recall patients in target age groups for initial and repeat vaccines is effective and possible in all primary care clinics.
Role of government
Multiple models exist around the world for vaccine funding policies: co-pay percentages, fixed costs with subsidies, full funding or no funding at all. Any policy must be simple, and identifying who qualifies should not be overly complex. Although accepting incremental gains is important as we move forward, the only vaccine programs in the world that meet targets are fully funded. Funding for pertussis booster vaccine in older people is needed in Australia.
Maximising access to vaccination
Broadening the base of sites to access vaccine beyond general practice will help increase coverage. Nurse-managed public immunisation clinics, immunisation by pharmacists and immunisation clinics in nursing homes have all been successful in increasing coverage.11 Opportunistic settings have been used in other countries, including an influenza vaccine van in the car park before a major football game in the US city of Seattle and immunisation clinics in supermarkets.
Recording, monitoring and evaluating vaccine programs in older people
To ensure improvements in vaccination programs for older people, program targets should be set and linked to monitoring and surveillance systems for both the disease and vaccination coverage. In particular, recording the burden of disease and its personal and financial impacts is crucial for obtaining financial support for programs.
Accurate recording of the time of vaccine administration is important for developing a recall system, measuring vaccine coverage, monitoring vaccine safety and providing payments for providers.
Conclusion
The uptake of vaccination in older people is suboptimal but attracts little focus at present. A move to a whole-of-life approach to immunisation and acknowledgement that preventive health care should be fair and equitable for all are needed. A national strategy should be developed that incorporates improved messaging about the risks versus benefits of vaccination and better data on vaccine coverage as well as disease incidence and outcome. The public messaging strategies should be freely available for use by other organisations and suitable for multiple-use formats. For example, enabling groups such as Diabetes Australia, the Heart Foundation and others to use pre-developed messages with their constituencies will aid message dissemination.
An increased focus on vaccination is needed in primary care, as well as better linkages between vaccination activities there and in other settings such as pharmacies. Targets for improved outcomes should be set and monitored. MT
References