Common vitreoretinal interface disorders. Detachments, holes, puckers and cysts

The vitreous is at the root cause of numerous retinal conditions, including retinal detachment, macular hole, vitreomacular traction and epiretinal membrane. The advent of optical coherence tomography has dramatically increased our understanding of the pathogenesis of these conditions and helped to improve surgical management.
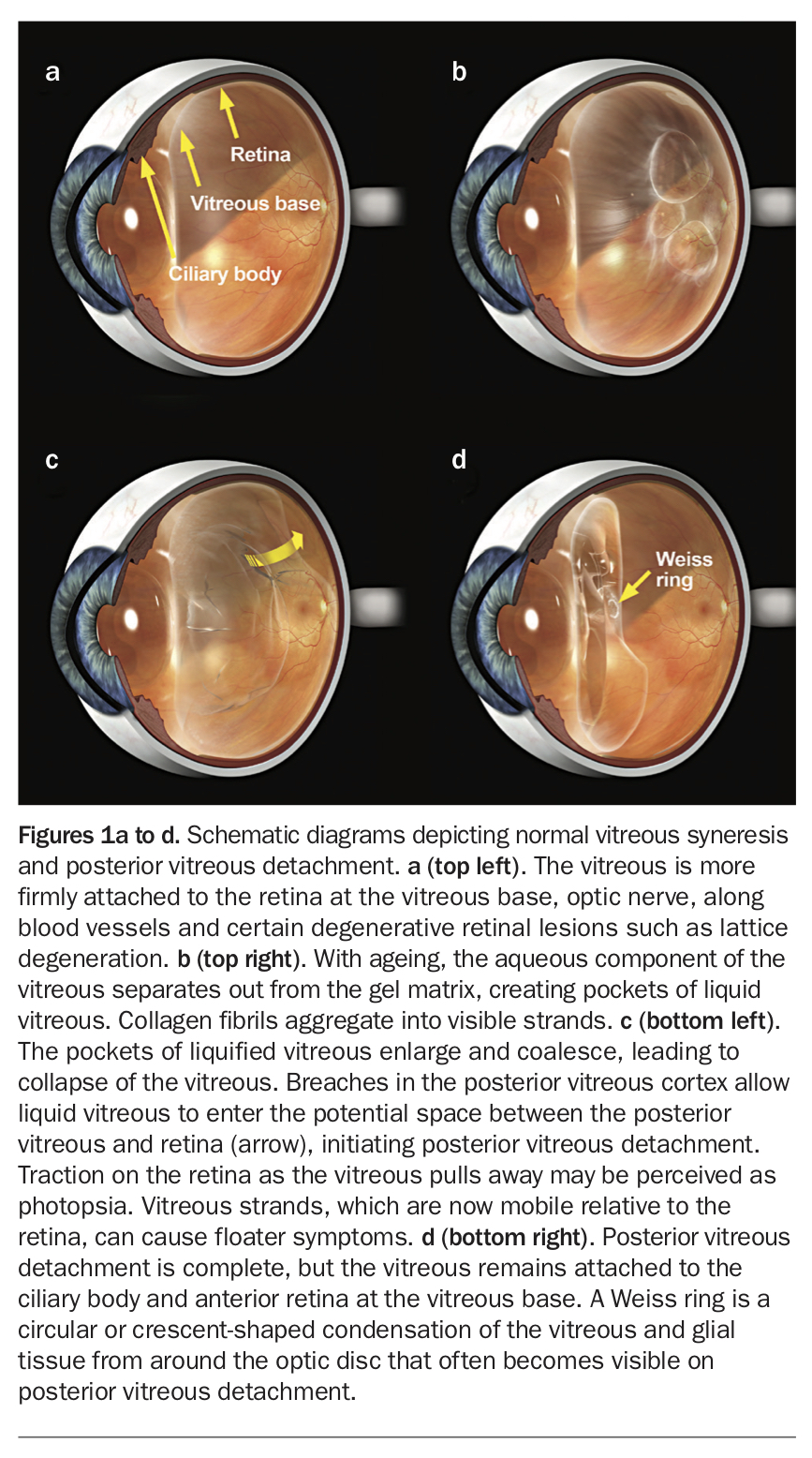
The vitreous fills the space in the eye between the lens and retina, occupying 80% of the internal volume of the globe. It is a transparent, avascular and mostly acellular gel consisting of 99% water, proteins, glycosaminoglycans and small amounts of salts and metabolites.1 It has a denser cortex and more liquid centre. The anterior part of the vitreous is permanently attached to a 4 to 6 mm annulus of retina and ciliary body, and is termed the vitreous base (Figure 1a). Posteriorly, the vitreous is relatively loosely attached, but the adhesion is firmer at the optic disc, at the macula, along blood vessels and over abnormal retinal lesions such as lattice degeneration.2 This is a key concept in understanding the pathogenesis of vitreoretinal interface disorders.
{kind=link}
Ageing of the vitreous and posterior vitreous detachment – flashes and floaters
The vitreous shares similarities with most extracellular matrices. It contains a network of collagen fibrils to which glycosaminoglycans (mainly hyaluronate) are attached that attract and hold water to form a gel matrix.1 The vitreous is transparent because of the even dispersion of the collagen fibrils. With ageing, the collagen fibrils tend to aggregate into larger bundles, which eventually become insoluble and form visible strands that can cause floater symptoms. The aqueous component of the vitreous separates out to form pockets of liquid vitreous that progressively enlarge (Figure 1b). This process is called syneresis, and floaters that appear over a long period are harmless as a rule.
Syneresis continues until, eventually, most of the vitreous becomes liquid, causing it to collapse (Figure 1c). Breaches in the vitreous cortex allow the liquid vitreous to enter the potential space between the vitreous and retina, initiating posterior vitreous detachment (PVD). Agitation of the vitreous induced by eye and head movements promotes vitreous separation. Photopsia may be perceived if there is sufficient traction on the retina as the vitreous pulls away. The typical arc-shaped flashes in the temporal visual field experienced by many individuals probably are due to the vitreous pulling away from the retina around the optic disc. The detached vitreous is more mobile relative to the retina, casting moving shadows that may be interpreted as new floaters (Figure 1d). A ring or crescent-shaped floater is called a Weiss ring, which represents condensed vitreous and glial tissue from around the optic disc margin. Although symptoms associated with such floaters usually settle with time, large floaters may be amenable to laser treatment.3
Abnormal posterior vitreous detachment
Because the vitreoretinal adhesion weakens with age, the posterior vitreous usually separates without causing significant traction on the retina. If this is not the case, the separation of the vitreous can exert stress on the retina and result in tractional damage.2 Premature PVD commonly seen with myopia, trauma, inflammatory conditions and intraocular surgery carries a higher risk of retinal detachment due to the still adherent vitreous.
Areas where vitreoretinal adhesion is naturally stronger become stress points during PVD. The macula is particularly susceptible because of firm vitreomacular adhesion and the thinner foveal tissue. Persistent traction can lead to oedema, splitting of the internal layers (schisis), tractional detachment or formation of a hole, resulting in a reduction of central visual acuity. In the peripheral retina, PVD can exert traction on the blood vessels causing haemorrhage and floater symptoms. Mild vitreous haemorrhage is common during PVD and is a clinical sign that warrants a thorough inspection of the retina for breaks. Retinal breaks can develop anywhere in the retina, but they are more likely to occur at certain degenerative lesions such as lattice degeneration. This is because the retina is thinner at these lesions and the vitreous is more adherent.4 If the lesions are judged to pose significant risks of retinal detachment, prophylactic retinopexy may be considered.
Uveitis, trauma and vascular disorders, such as diabetic retinopathy and retinal vein occlusion, can promote growth of scar tissue at the vitreoretinal interface, which may increase vitreoretinal adhesion. Retinal neovascularisation can extend into the vitreous, posing a threat of vitreous haemorrhage. Neovascularisation may result in tractional scars that can ultimately cause retinal detachment.
Retinal detachment
Most acute retinal detachments are rhegmatogenous, meaning they result from retinal breaks. Retinal detachment occurs with an annual incidence of around one in 10,000, and the lifetime risk is estimated to be one in 300.5 Acute retinal detachment is a medical emergency. Symptoms of early retinal detachment are identical to uncomplicated PVD, which is why all individuals experiencing an acute onset of flashes and floaters should be examined without delay.
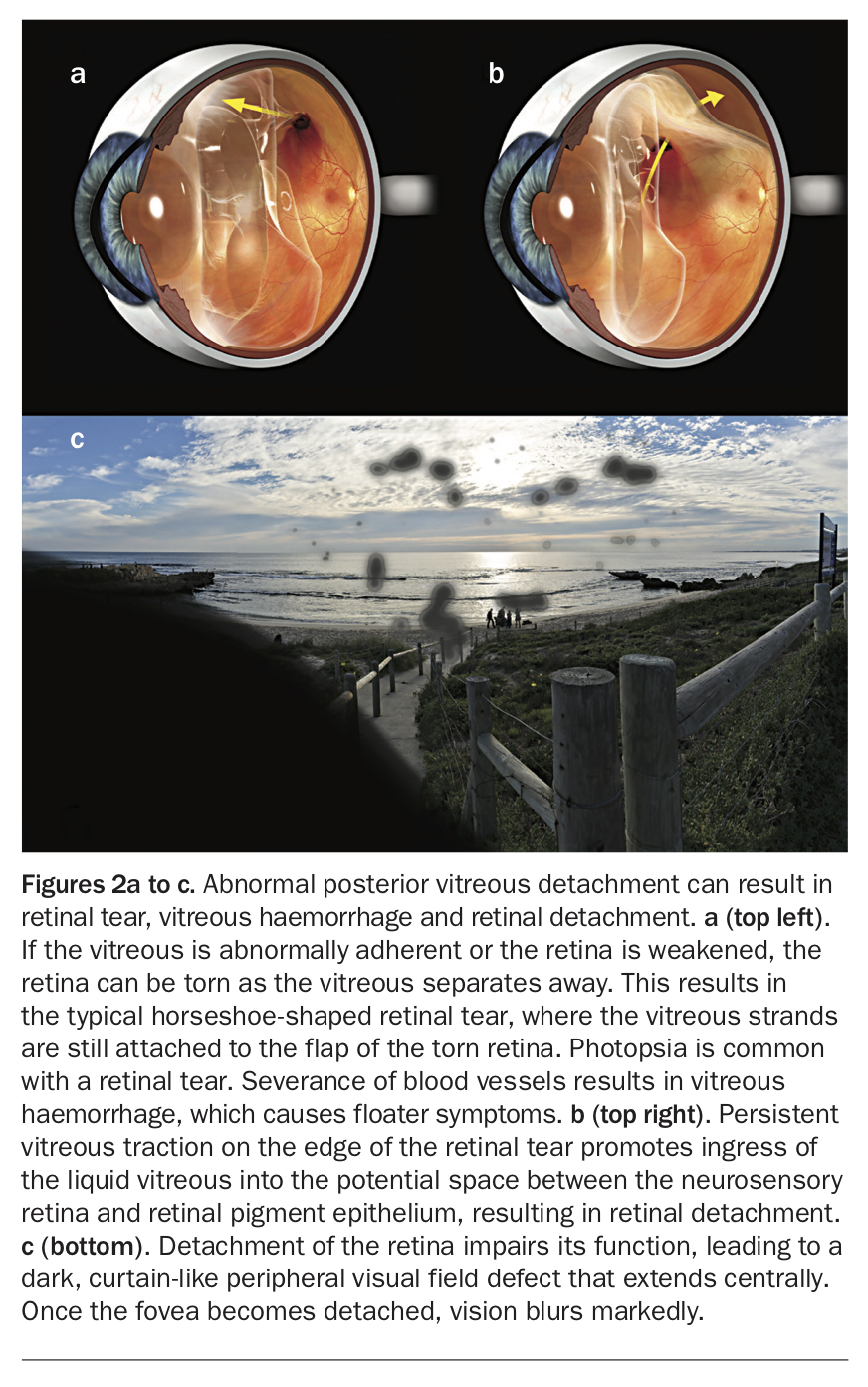
When the retina is torn, the strands of vitreous still attached to the flap of the tear exert ongoing traction induced by eye movements (Figure 2a). This has the effect of promoting the entry of fluid into the subretinal space, initiating retinal detachment (Figure 2b). As the detachment extends, a peripheral field defect may be perceived (Figure 2c), which expands centrally until the fovea is detached. At this point, vision usually deteriorates markedly and appears distorted. Once the fovea detaches, some permanent visual impairment is unavoidable. Macula-sparing retinal detachment is therefore treated as an emergency.
{kind=link}
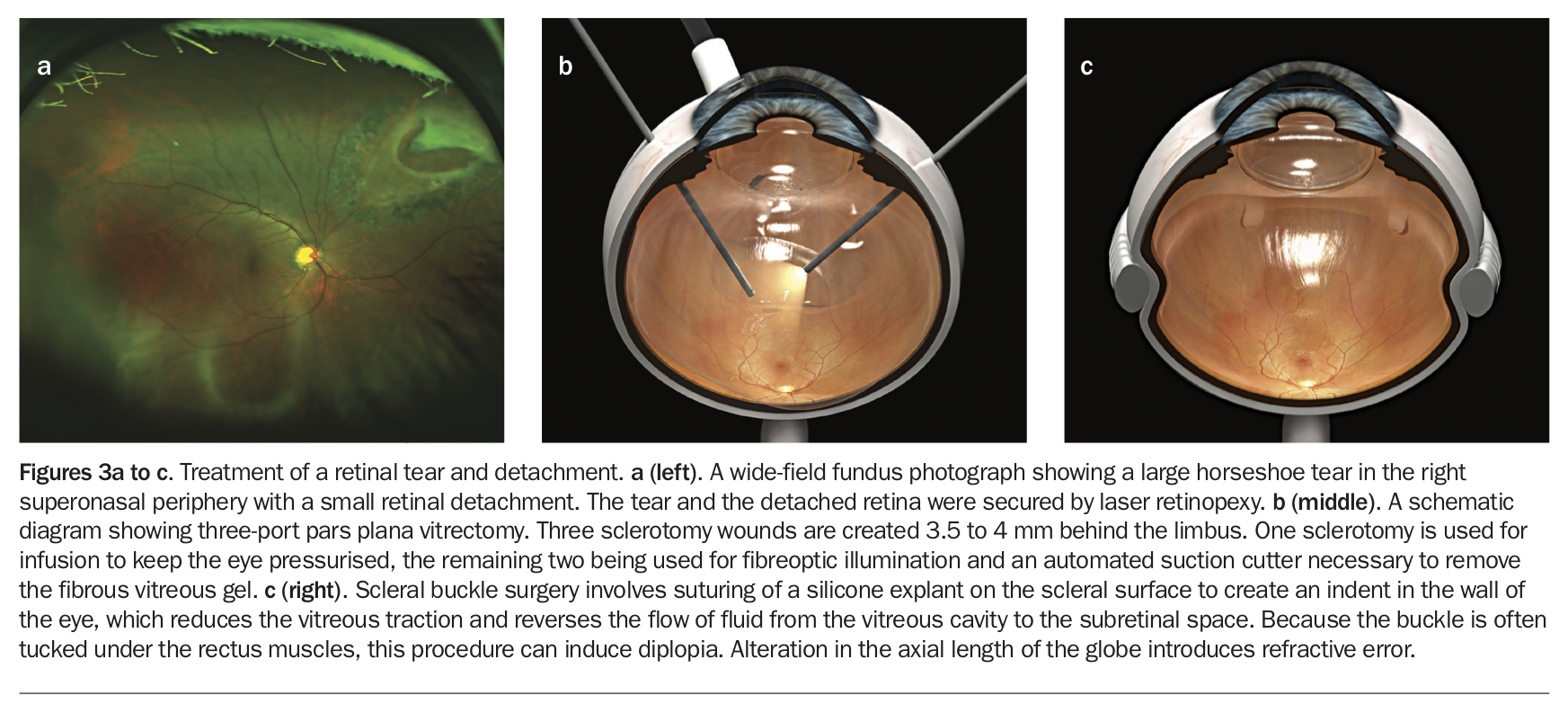
The best time to treat retinal detachment is before the detachment enlarges. If there is only a small volume of subretinal fluid around the break, further extension can be stopped by applying barrier laser photocoagulation or cryopexy (Figure 3a). However, larger areas of subretinal fluid cannot be managed with retinopexy alone, necessitating surgical reattachment of the retina.
{kind=link}
Established retinal detachment can be repaired by vitrectomy or scleral buckle surgery, and there are pros and cons for each approach (Figures 3b and c). Both are usually performed under local anaesthesia. Vitrectomy is quicker, causes less discomfort, does not disrupt extraocular muscles and clears the vitreous opacities. However, it has an important disadvantage of promoting cataract formation. Gas tamponade is usually administered, and postoperative head positioning may be required. Air travel is strictly forbidden when gas is in the eye. Scleral buckle insertion is sometimes misunderstood to be a superseded technique, but it remains the best approach for young patients with inferior retinal detachment. Complex retinal detachments may require both vitrectomy and scleral buckle surgery.
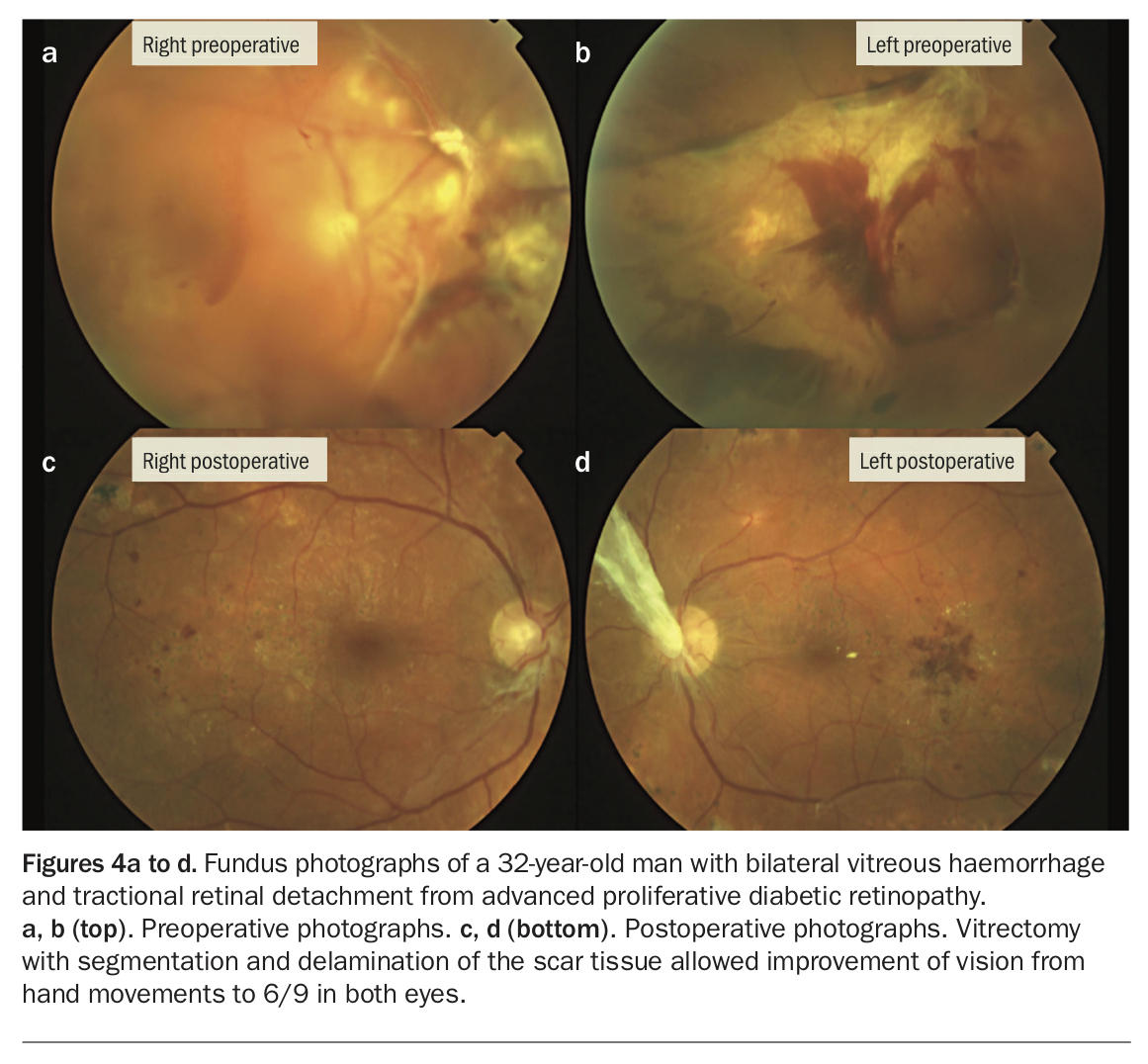
Tractional retinal detachment is usually managed nonurgently, except when a break converts the detachment into a rhegmatogenous type. Persistent traction from contracting bands of scar tissue leads to elevation of the neurosensory retina from the retinal pigment epithelium. Visual acuity deteriorates when the macula becomes involved or when concurrent vitreous haemorrhage develops. Tractional retinal detachment is usually managed via vitrectomy to cut and remove the traction bands, allowing the detached retina to settle (Figures 4a to d).
{kind=link}
Vitreous haemorrhage
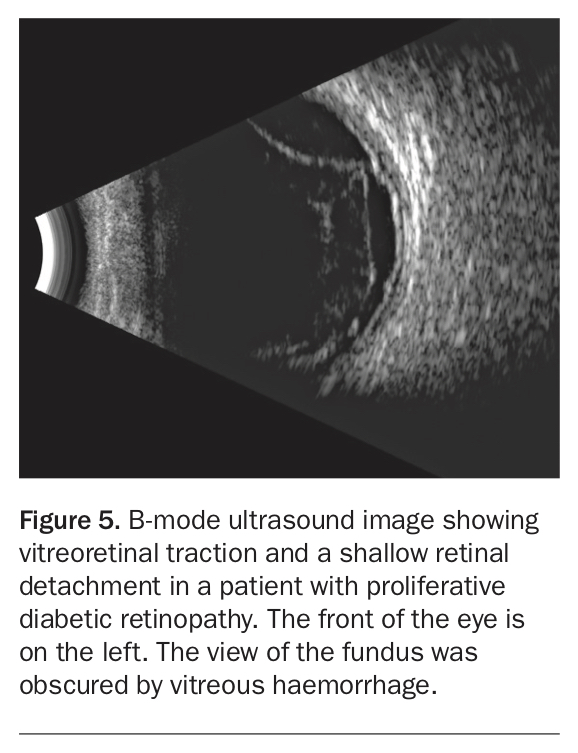
Vitreous haemorrhage is usually first noticed as hair or cobweb-like strands of floaters, which disperse and blur the vision. If bleeding continues, vision can be profoundly reduced and the dense haemorrhage can preclude adequate examination of the retina. B-mode ultrasonography is useful in examining the posterior segment when ophthalmoscopy is not possible, but it is not sufficient to exclude retinal tears (Figure 5).
{kind=link}
There may be likely reasons for vitreous haemorrhage. For example, in a patient with proliferative diabetic retinopathy, it is likely that the bleeding occurred because of vitreous traction at neovascular fronds. If severe vitreous haemorrhage occurs in a patient without pre-existing retinopathy, vitrectomy and exploration may be indicated because the likelihood of a retinal tear is high. Provided the bleeding ceases, vitreous haemorrhage can resolve fairly quickly. However, recurrent or persistent haemorrhage can cause significant morbidity and prevent treatment of the causal problem, in which case vitrectomy would offer the most expeditious restoration of vision.
Vitreomacular interface disorders
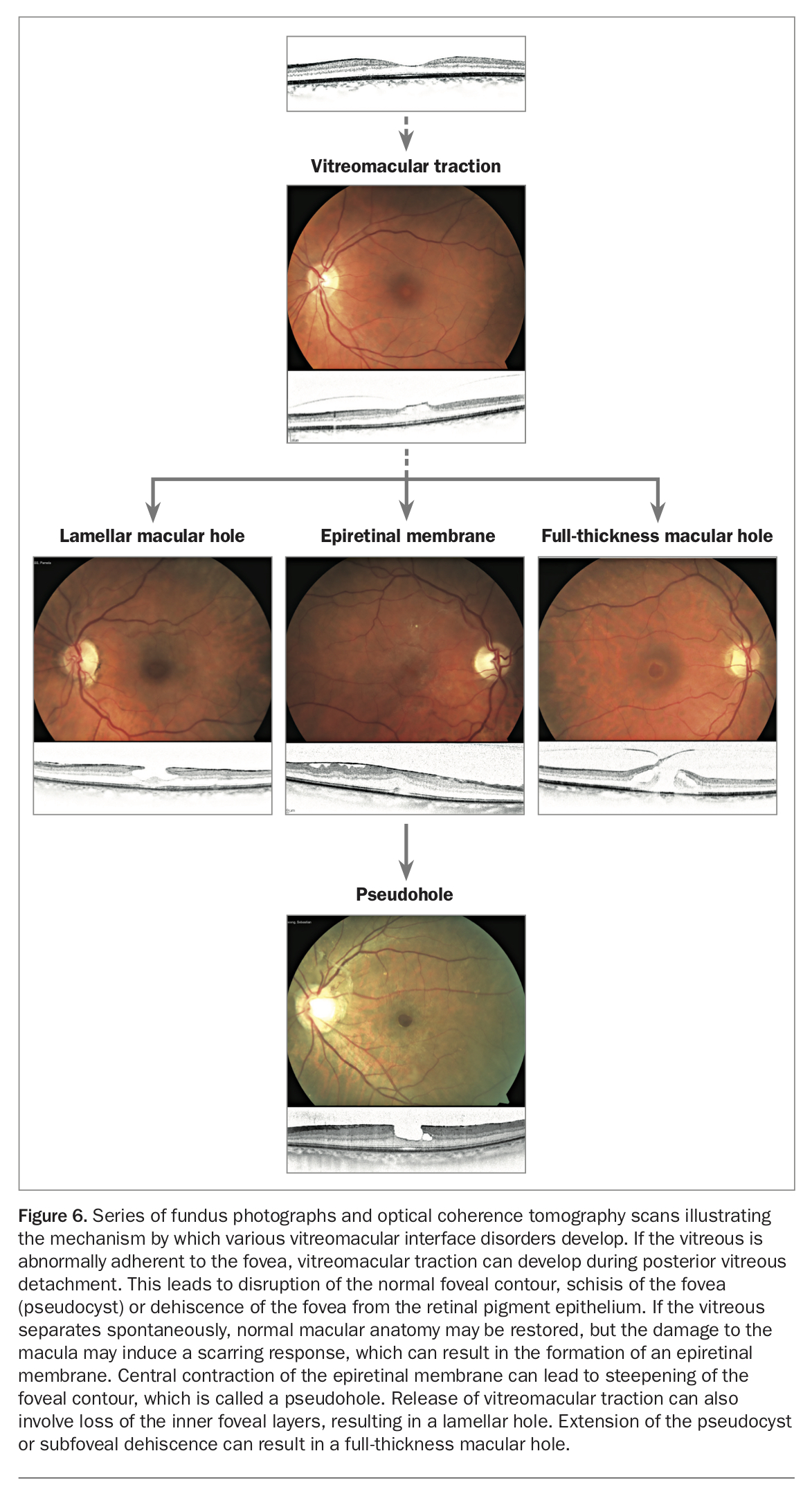
Anomalies at the interface of the vitreous and macula can manifest in various ways, but they share similar pathogenesis and treatment approaches (Figure 6). Common vitreomacular interface disorders include epiretinal membrane or macular pucker, vitreomacular traction and macular hole. Vision loss is usually gradual. High-resolution optical coherence tomography (OCT) is indispensable for accurate diagnosis and follow up of these conditions. This imaging technique uses a broad-band light source to sample reflected light from a retinal locus, which is compared with a reference light via interferometry (A-scan). Adding many A-scans to build a cross sectional image of the retina produces a B-scan, which is the most common mode of use of OCT.
{kind=link}
Epiretinal membrane
Epiretinal membrane refers to proliferation of fibroglial scar tissue on the surface of the macula. It first appears as a reflective sheen, which thickens to a pale membrane over the macular surface. Contraction of the membrane can lead to swelling and puckering of the underlying macula, resulting in visual blurring and distortion. It is unusual for an epiretinal membrane to cause severe vision loss, but a moderate degree of visual impairment is common. Most epiretinal membranes are idiopathic, thought to result from PVD stimulating an inflammatory scarring response. In a minority of cases, there are underlying aetiologies such as diabetic retinopathy, retinal vein occlusion, uveitis or trauma, which promote inflammation and scar formation.
Epiretinal membranes are common, with a five-year incidence greater than 5% among individuals older than 49 years of age.6 Fortunately, intervention is not necessary in most patients because the scarring process is limited and can improve spontaneously. When the macular oedema and distortion prove to be progressive and cause visual symptoms, surgical removal of the epiretinal membrane is indicated. Complete restoration of vision is usually not possible, which is the reason for the recent trends for earlier intervention. If the macula contracts centrally to steepen the foveal wall, the appearance can resemble a macular hole (pseudohole).
Vitreomacular traction
Vitreomacular traction is the disturbance of central macular anatomy or function due to persistent vitreous pull. Abnormally adherent vitreous typically manifests as persistent attachment of vitreous cortex at the fovea, while it has separated from the surrounding macula. The changes may be subtle, with only a mild kink visible in the normally U-shaped foveal cross-section. However, the traction can lead to a more significant disruption, leading to schisis at the fovea (pseudocyst) or elevation of the sensory macula from the retinal pigment epithelium.
In the absence of symptoms, there is a good likelihood of the vitreous separating spontaneously, which should lead to restoration of normal macular anatomy and function. However, only one in 10 cases of symptomatic vitreomacular traction have been shown to resolve spontaneously after five years.7 The symptoms include visual blurring, distortion and a relative scotoma at fixation. Vitreomacular traction can progress to a full-thickness or lamellar macular hole and result in a significant vision loss. Surgery is therefore considered for symptomatic cases or when reduction in vision can be demonstrated.
Lamellar macular hole
Lamellar macular hole can develop if the vitreous pulls away, taking with it the inner layers of the central macula. The resulting defect appears as a round or oval dark spot at the fovea, often with an irregular border. Visual acuity is usually mildly reduced but a more severe loss is possible. Because there is no persistent vitreous traction, vision and macular anatomy tend to stabilise. Most cases of lamellar hole are managed conservatively, but follow up is recommended because they may progress to full-thickness macular holes or develop an epiretinal membrane, which can threaten vision.
Full-thickness macular hole
Full-thickness macular hole is relatively common, with a prevalence of 0.4% among individuals older than 60 years.8 Women are more frequently affected than men. It usually develops from persistent vitreomacular traction leading to the opening of a full-thickness macular defect, but it can also develop without vitreous traction, presumably through a tangential force pulling the hole open. It can also develop from a pre-existing lamellar hole. A round or oval punched-out hole can be seen ophthalmoscopically. Full-thickness macular holes usually cause central scotoma, as well as distortion and visual blur. It has a poor natural history; vision deteriorates to the level of legal blindness in most cases without intervention. Spontaneous hole closure is unlikely.9 Recent-onset full-thickness macular holes are readily treatable, with an anatomical success rate approaching 100%. Older holes have reduced closure rates and poorer visual outcome. Surgery is recommended for all patients with recent-onset full-thickness macular holes.
Management
The standard treatment for vitreomacular interface disorders is vitrectomy. Recent advances in technology and surgical techniques have made vitrectomy much safer. Acceleration of cataract formation remains a major disadvantage. Because of this, surgery is offered to patients who have suffered visual impairment, or in whom progression is demonstrable with a high likelihood of vision loss. On the other hand, long-term visual outcome is superior when the surgery is performed before the macula has sustained significant damage.
A complete vitrectomy and induction of PVD is sufficient to address most vitreomacular tractions. Pharmacological liquefaction and induction of PVD is possible with intravitreal injection of ocriplasmin, a protease subunit of human plasmin. However, its efficacy is significantly lower than vitrectomy, with resolution of vitreomacular traction and full-thickness macular hole closure achieved in less than 50% of cases.10
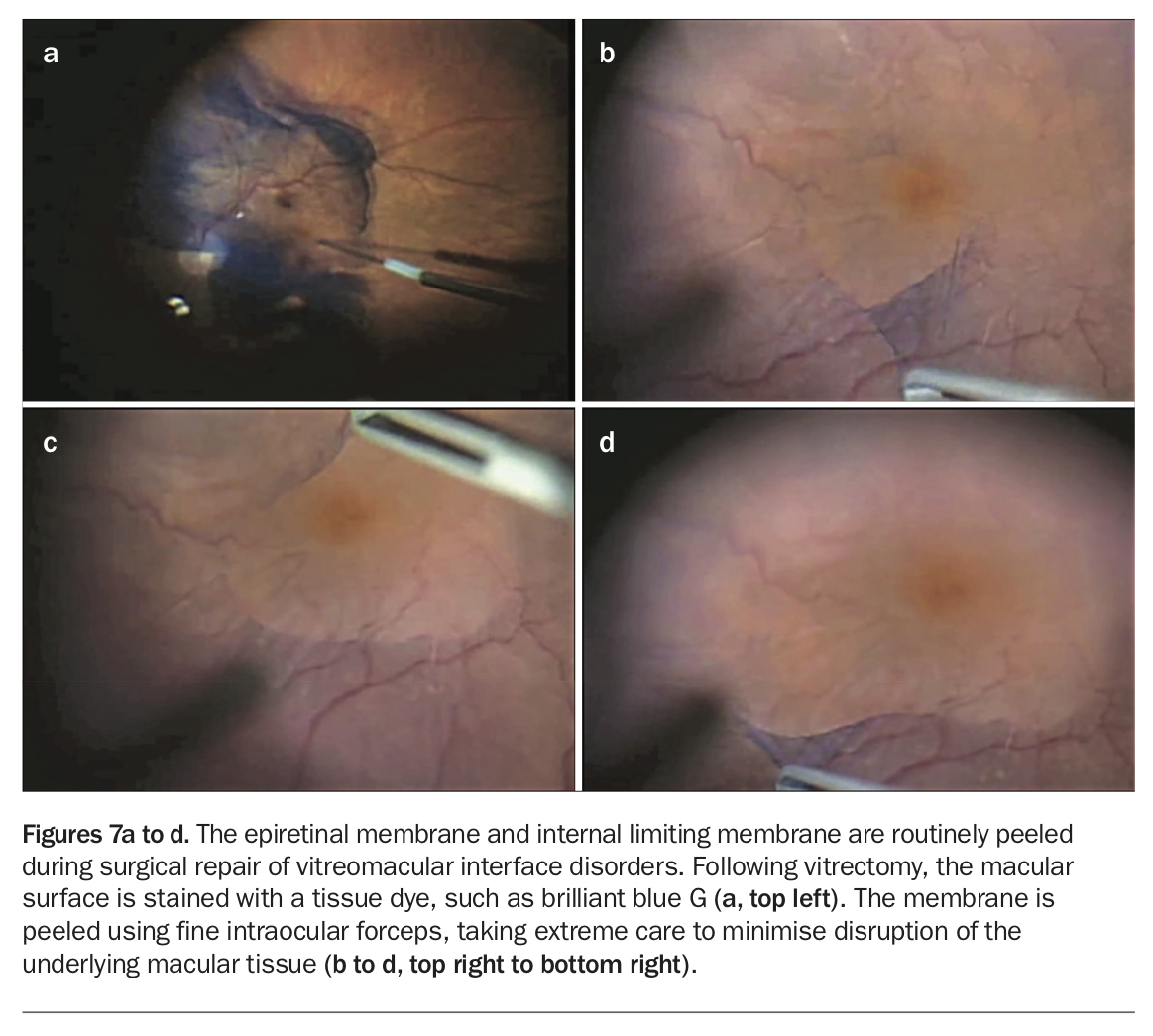
The epiretinal membrane is peeled using intraocular forceps with the aid of a tissue dye (Figures 7a to d). The internal limiting membrane is peeled for repair of macular holes, for which gas tamponade is administered to aid hole closure. Strict prone positioning is less commonly enforced but the patient is encouraged to avoid lying flat on their back and must not travel by air while the gas is in the eye.
{kind=link}
Modern, minimally invasive, sutureless, small gauge vitrectomy causes minimal discomfort and recovery is rapid. Postoperative pain is unusual and must be investigated. Overall, the surgical risk profile is comparable to that of cataract surgery. It includes endophthalmitis (one in 2000 to 5000), retinal detachment (one in 200 to 500), bleeding and postoperative ocular hypertension or hypotension.11 There is also a risk of vision loss through anaesthetic complications. Cataract, the surgery for which is usually highly successful, should not be considered a risk, but rather a side effect of vitrectomy.
Conclusion
The role of abnormal vitreoretinal interface in the pathogenesis of common retinal conditions is increasingly appreciated and understood. Advances in vitreoretinal surgery offer safe and effective means of intervention for patients with visual impairment. Some conditions, such as retinal detachment, need urgent management, although unnecessary delays should be avoided even for macular conditions which may prove to be stable. It is important to remind patients that visual impairment should not necessarily be attributed to cataract or simply old age. A thorough evaluation is advised if a significant change in vision is perceived. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.