Constipation. How to get started

Constipation is one of the most common gastrointestinal conditions presenting to general practitioners. Investigations are required in only limited cases, and keys to management include appropriate education, alteration of lifestyle factors, good communication, sometimes pharmacological therapy and rarely, more invasive treatments.
Remember
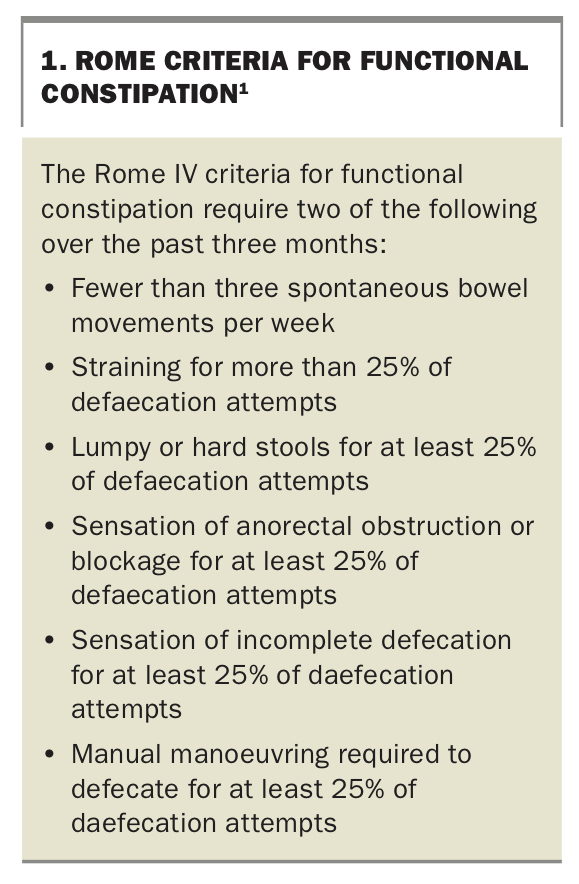
- Most, if not all, adults have experienced constipation at some stage in their lifetime. An international group of experts have developed consensus criteria that can be used in research and in clinical practice to make the diagnosis of constipation (Box 1).1
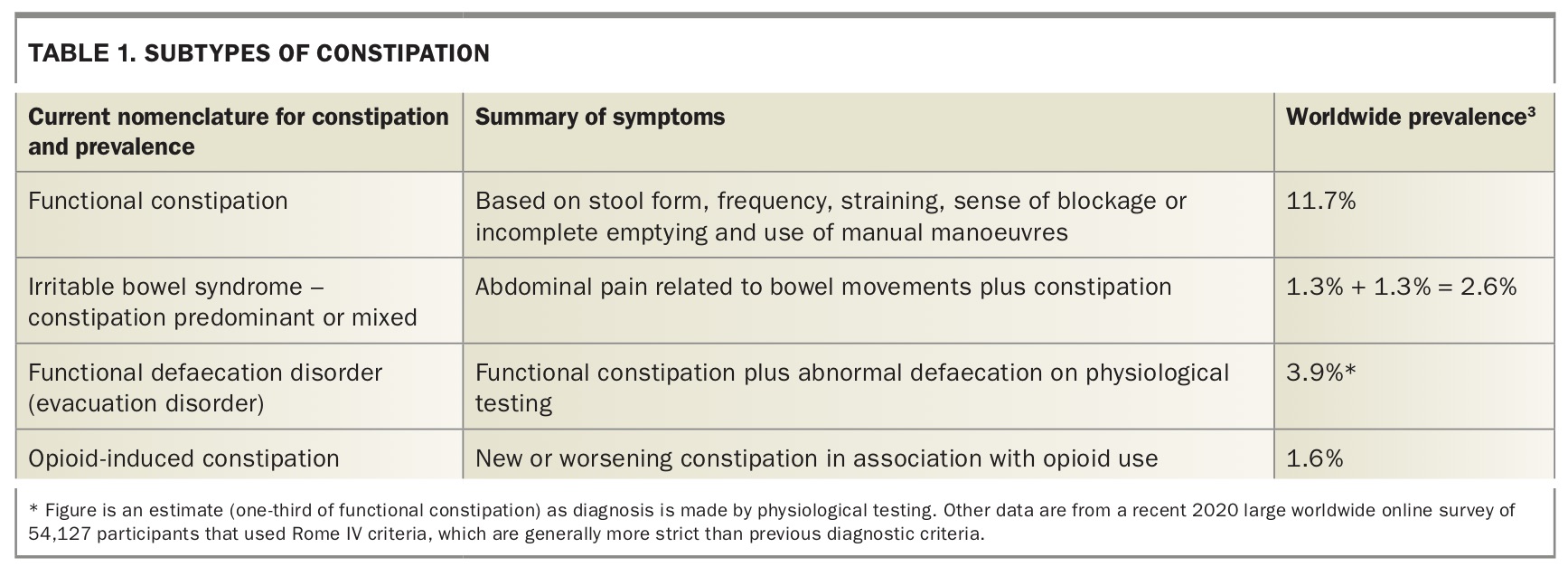
- If constipation is accompanied by abdominal pain related to bowel habit, it is termed constipation-predominant irritable bowel syndrome (IBS). Subtypes of constipation are summarised in Table 1.
- If constipation is accompanied by evidence of poor rectal evacuation the term ‘functional defaecation disorder’ can be used.1 Symptoms that are more suggestive of an evacuation disorder include incomplete emptying, excess straining, feeling of a blockage, and digitation or use of manoeuvres to facilitate evacuation.
- Opioid-induced constipation affects 40 to 80% of all opioid users and has an increasing prevalence in society.2,3
- Chronic constipation is a highly prevalent condition, affecting 10 to 15% of the population. Prevalence was previously thought to rise with age; however, this was not borne out in the largest study to date (54,127 online participants) in which people over 65 years of age had similar if not slightly reduced prevalence compared with 40 to 64-year-olds and 18 to 49-year-olds.3 It is possible that immobile, elderly nursing home residents who may experience high rates of constipation were under-represented in this internet questionnaire-based study.
- In the same large study, the female preponderance of constipation was confirmed (15.2% of women, 8.3% of men).3
{kind=link}
{kind=link}
Assessment
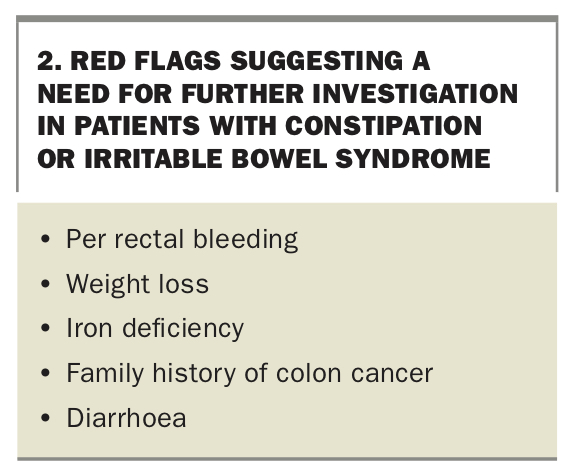
- Clinical evaluation by history taking to determine the exact nature and degree of burden of symptoms is essential, as well as excluding the presence of any red flags such as rectal bleeding, family history of colon cancer, anaemia, iron deficiency or weight loss (Box 2).4
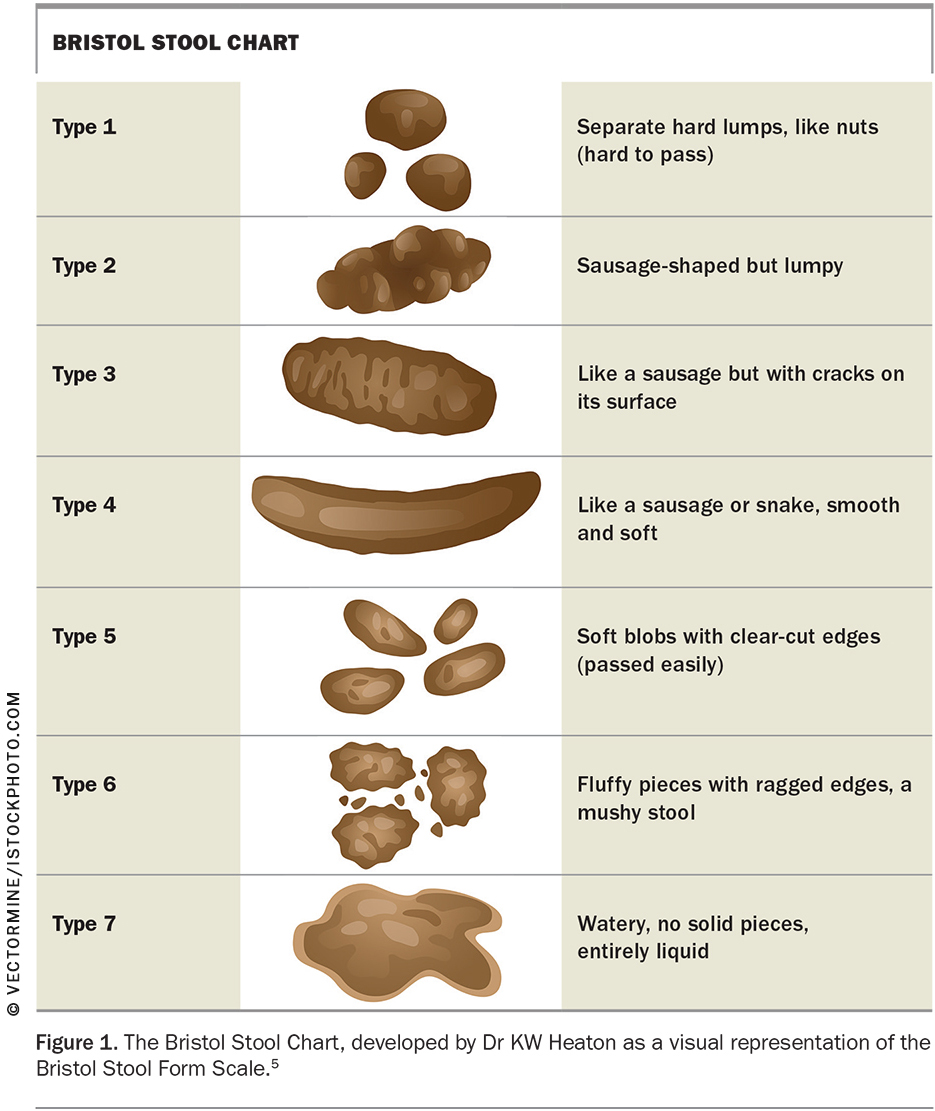
- Patients and doctors mean different things by the word ‘constipation’ and it is important to ask the patient specifically what they mean. Do they have hard stools, infrequent stools, straining, abdominal pain or a feeling of incomplete emptying? It can be useful to show a picture of the Bristol Stool Chart to assist patients in describing their poo (Figure 1);5 and use of a bowel diary is more effective than self-reporting in determining the results of any therapeutic intervention.6
- Medications and other medical conditions associated with constipation should be noted and considered (e.g. calcium channel blockers, iron supplements, diabetes, Parkinson’s disease).
- Faecal incontinence commonly coexists and should be specifically enquired about as patients are often reluctant to volunteer this symptom.
{kind=link}
{kind=link}
Investigations
- Determining who needs a colonoscopy is an important question in each patient’s assessment and there is no evidence that chronic constipation is a risk factor for the development of colorectal cancer, despite popular belief.7 Those not requiring colonoscopy should be reminded to undergo a faecal occult blood test two-yearly if over 50 years of age, as per current Australian guidelines.8
- Patients should be screened for coeliac disease, particularly if they additionally have irritable bowel syndrome or any risk factors for coeliac disease such as type I diabetes, autoimmune thyroiditis or family history.
- Rarely, screening for hypercalcaemia and hypothyroidism may be indicated and iron studies may be useful as the presence of iron deficiency may highlight the need for colonoscopy (and endoscopy).
- Abdominal examination should be performed and may suggest fullness due to faecal loading, especially in the right iliac fossa (caecum) or sigmoid area. A digital rectal examination should be performed to assess for evidence of an evacuation disorder. If this is suspected, further investigation with high-resolution anorectal manometry may be warranted, especially if initial simple management has failed.
- Abdominal x-ray can be used to assess for the degree of faecal loading if this is unclear after clinical evaluation, especially if there is coexistent faecal incontinence and constipation with overflow is suspected. If moderate or marked faecal loading is present the dose of laxatives may be adjusted accordingly.
- Colonic transit studies using Sitz markers or nuclear medicine can be performed to diagnose a subset of patients with slow transit constipation but do not often alter management other than in the more severe cases of constipation when surgery is being considered.
- A defaecating proctogram is a test in which patients are asked to expel a barium-containing artificial stool over a commode under x-ray screening to look for structural problems in the pelvic floor and anorectum. This test is usually reserved for those who have failed conservative management including biofeedback and should be interpreted with some caution as some findings are present in both symptomatic and asymptomatic individuals.
Management
Not all patients with constipation require treatment; however, when symptoms are troublesome, a stepwise approach is reasonable starting with diet and lifestyle factors, fibre supplementation followed by addition of medications (Table 2) or consideration of biofeedback if necessary. Providing patients with a management plan in writing may enhance adherence.
{kind=link}
Dietary and lifestyle modification
- Water. Ensure adequate noncaffeinated, nonalcoholic beverage intake (NHMRC guidelines are 2.1 L daily for women and 2.6 L daily for men, or more with exercise). There is no evidence that higher volumes provide benefit.9
- Fibre. Increase dietary fibre towards the recommended 25 g (for women) to 30 g (for men) daily (as most people consume below the recommended level).9 This improves stool form and stool transit and is better tolerated if slow increments are made over some time.10
- Exercise. Given that exercise is generally beneficial, it may be recommended in patients with constipation, although there is only low-level evidence supporting its efficacy, mainly in older patients and those with coexistent IBS.
- Sleep. Again, given the general benefits of getting enough sleep and very low-level evidence to support that gastrointestinal symptoms may be worse after a poor night’s sleep (mainly in IBS), advice for obtaining adequate sleep is reasonable.
Toileting behaviour
- Recommend taking advantage of the gastrocolonic response by not skipping meals, avoiding prolonged fasting and attempting defaecation after a meal.
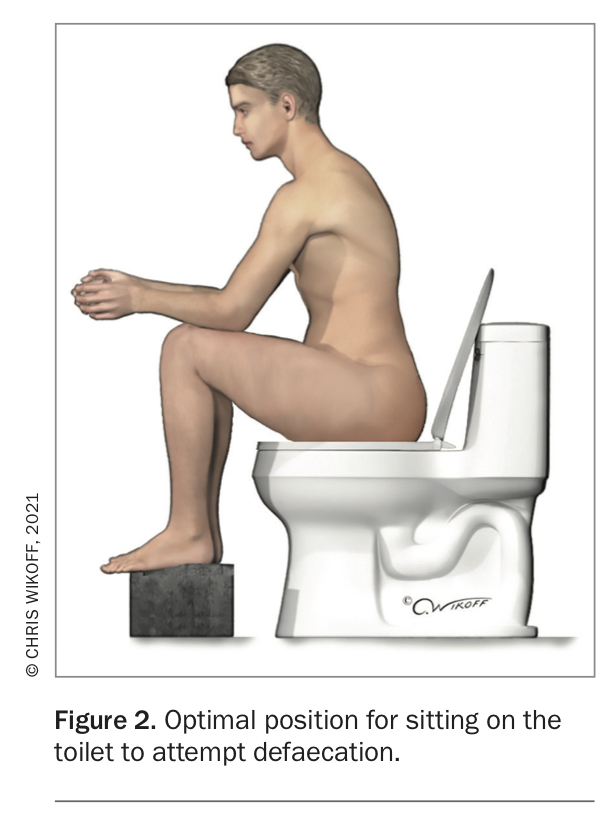
- Use of footstool: Encourage patients to keep a footstool in their bathroom to place their feet on while attempting defaecation. The recommended position is to have knees higher than the level of the hips and to slightly lean forward (Figure 2).
{kind=link}
Supplemental fibre
- Often supplemental fibre is useful in combination with (or sometimes instead of) an increase in dietary fibre to treat constipation, particularly with the goal of normalising stool form. A normally formed stool can be evacuated much more easily than a loose or hard stool. It can be worthwhile beginning at a very low dose (even as little as half to one teaspoon) and increasing the dose according to the degree of bloating, stool form and intercurrent dietary fibre intake.
Osmotic agents
- Low-dose polyethylene glycol. This is the current mainstay of treatment because of its safety profile and high-quality evidence of its efficacy. It works as an osmotic agent, drawing water into the colon and increasing stool frequency and improving stool form. Some helpful tips with prescribing polyethylene glycol include:
– the effect may not be as predictable as with a stimulant laxative, and it is helpful to explain to patients that osmotic agents have a less immediate yet more ‘overall’ effect
– patients may initially feel some bloating or discomfort until the bowel movements start increasing, but with time the dose is better tolerated and symptoms reduce
– the dose should be titrated to stool form.
- Other osmotic agents that can be used include the nonabsorbed sugars lactulose or sorbitol (which may possibly cause more bloating), or magnesium (such as Epsom salts, yet this may cause more unpredictable, watery stool).
- Stimulant laxatives: Controversy exists surrounding the use of stimulant laxatives (e.g. senna, bisacodyl, cascara). They do cause high amplitude contractions in the colon and predictable bowel movements after taking them. They do cause melanosis coli seen at colonoscopy. They have been linked with possible dependency and a dilated atonic colon after many years of use (often more than 20 years). For these reasons, they may not be the best choice for young patients but may be good choices for older patients or for short-term use (e.g. after surgery). Stimulant laxatives come in many different forms including herbal treatments, teas and over-the-counter medications. The challenge for doctors (and patients) can be to identify the presence of stimulants, as there is a variety of formulations with variable use of labelling.
- Softeners/emollients. Stool softeners such as docusate are commonly used to treat constipation; however, evidence is lacking regarding their efficacy. Small doses of supplemental fibre such as sterculia or psyllium (e.g. one to two teaspoons) may be preferred to optimise stool form.
Per rectal therapies
- Enemas and suppositories. Osmotic-based enemas (e.g. Microlax, sodium phosphate) and glycerol suppositories are an underutilised therapy for constipation. They are used more extensively in other parts of the world (e.g. Europe) and can give the patient great predictability in their bowel emptying, which can be a significant advantage (especially those patients with both constipation and faecal incontinence). They can be used regularly or as needed.
- Rectal irrigation. This procedure is usually performed for severe cases of constipation, especially in the context of neurogenic bowel.
Prucalopride
- Prucalopride is a 5-HT4 receptor agonist available in Australia for management of chronic constipation in patients who have not had adequate relief from other laxatives. It comes in 1 and 2 mg tablet dosage with both doses being moderately efficacious.
- Headache is the most common side effect and sometimes precludes ongoing use. Expense limits use for some patients, and if there is no improvement after one month it probably should not be continued.
Future medications
- Linaclotide. This is a guanylate cyclase C agonist, which is luminally rather than systemically active, has a very favourable side-effect profile and is available in tablet form in the US and Europe. There is high-quality evidence showing its efficacy for constipation.
- Lubiprostone. This is a chloride channel activator that increases secretions and softens stool. There is high-quality evidence for its efficacy in constipation, but it is not available in Australia as yet.
Biofeedback or pelvic floor physiotherapy
- For patients who are refractory to standard management, or those with dyssynergic symptoms such as incomplete emptying, excess straining, prolonged toileting time or digitation, anorectal manometry with a view to biofeedback is indicated. During this treatment, patients are usually given visual feedback about the rectal pressure they create when pushing on the toilet, as well as their anorectal and pelvic floor musculature, and they are coached on how to normalise the defaecation manoeuvre. It is performed in specialised centres under the supervision of a colorectal surgeon or gastroenterologist. Pelvic floor physiotherapy is a very reasonable alternative, although is less specific and does not always involve ‘feedback’.
Surgery
- Surgery is rarely performed for constipation other than in carefully selected patients.
- Total colectomy and ileorectal anastomosis is rarely performed for management of slow transit constipation.
- Surgery is also occasionally performed in structural disorders of the pelvic floor (e.g. a large nonemptying rectocoele) that fail conservative treatment and biofeedback.
- Unlike for faecal incontinence, there is no role for sacral nerve stimulation in the treatment of constipation.
Conclusion
After performing a careful history and physical examination and determining the predominant symptom, only minimal testing is required for the evaluation of constipation. Initial therapy should involve lifestyle measures, fibre supplementation and osmotic laxatives. For those in whom these therapies fail, especially if there are symptoms of difficulty emptying the bowel, then anorectal manometry should be performed to look for dyssynergic defaecation, which can be treated with biofeedback. For those resistant to initial therapy, further options include increasing the osmotic agent or using newer pharmacological treatments such as prucalopride; psychological evaluation if appropriate; and per rectal therapies if they have not been tried. Surgery is rarely performed for constipation. MT