Osteoarthritis: moving beyond ageing

Osteoarthritis
Osteoarthritis is a heterogeneous group of diseases characterised by pain and loss of function, and is a leading cause of disability worldwide. Although risk factors vary across joints, common factors include obesity and advancing age. A largely clinical diagnosis, management for symptomatic disease is centred on nonpharmacological and nonsurgical measures.
- Osteoarthritis (OA) is the most common form of arthritis, and a leading cause of disability worldwide.
- OA is a heterogeneous disease with risk factors varying across different joints affected, although there are some shared risk factors (e.g. age, obesity).
- A clinical diagnosis can be made in the absence of red-flag features (e.g. prolonged early-morning stiffness).
- Nonpharmacological therapies are the mainstay of OA management and include exercise and weight loss; comprehensive assessment and regular review are also important features of therapy.
- Pharmacotherapy is ideally limited to the treatment of acute flares of pain; opiates are rarely indicated given an unfavourable risk-benefit profile.
- Joint replacement is reserved for advanced symptomatic disease; arthroscopy rarely provides clinical benefit.
Osteoarthritis (OA) is the most common form of arthritis, affecting 2.1 million people in Australia (9% of the population).1 OA is a significant cause of progressive pain and disability for the individual, leading to significant societal costs related to healthcare spending and disability.1 The burden of disease is expected to rise in our ageing population, with the increased prevalence of major risk factors for OA including obesity. GPs are usually the first point of contact and the main co-ordinating healthcare practitioner for patients with OA.
Common presentation
OA is a complex condition. Although it can affect any joint, it most commonly affects the hands, knees, hips, neck and feet. OA also commonly affects the back, although pathological and imaging changes, which are more common with advancing age, do not correlate well with clinical features.2
The most common presenting symptoms in patients with OA are pain and limitation of function. Joint pain can vary over time, but is often increased with or after activity. Morning stiffness may be present but generally lasts less than 30 minutes, an important feature differentiating OA from inflammatory arthritis. Bone swelling may be present over affected joints.
Most common causes
OA is a disease of the whole joint that is characterised by loss of articular cartilage and changes to surrounding bone. It is now clear that OA is not a single disease, but occurs as the result of varying combinations of multiple distinct but overlapping risk factors and pathological mechanisms, many with a systemic basis.3 Although the prevalence of OA across all joints increases with age, it is not an inevitable consequence of ageing: symptomatic disease is more closely related to other risk factors including obesity and psychological factors.4
Knee osteoarthritis
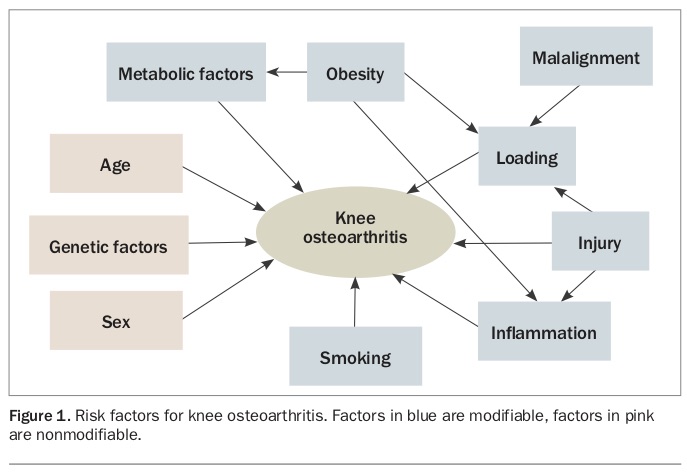
Risk factors for knee OA include ageing, female sex, family history, obesity, injury and malalignment (Figure 1).5 Although it is well established that obesity is a major risk factor for knee OA, over the past decade there has been a significant increase in understanding of the mechanisms by which obesity affects the knee. It is now clear that the effect is not simply through loading of the joint, but also through metabolically driven inflammation, associated with fat: fat is no longer viewed as an inert tissue, but the source of many inflammatory factors that have been shown to damage the knee.6 Therefore, obesity primes the joint by causing low-grade inflammation, making it more susceptible to damage by increased loads from a combination of higher weight and aberrant compensatory gait patterns that contribute to malalignment.
{kind=link}
Although high levels of physical activity are believed to be bad for joints, the effect of physical activity and subsequent risk of developing OA are dependent on the state of the underlying joint. This is partly due to joint inflammation associated with injuries. It is now clear that physical activity is important for maintaining healthy knee joints.
Hip osteoarthritis
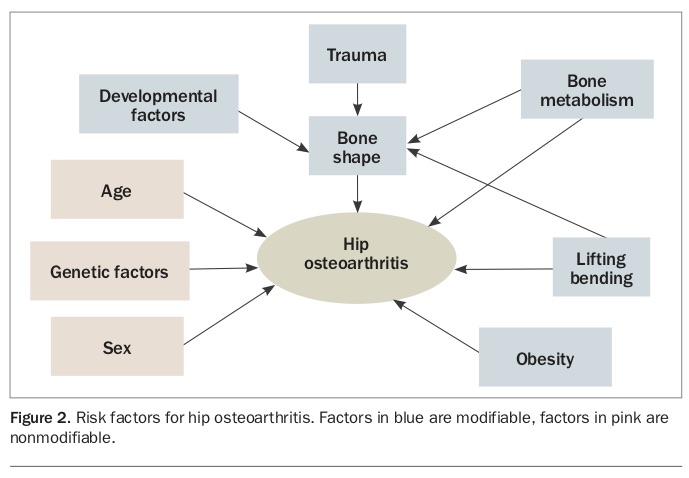
There is increasing evidence that hip OA is strongly influenced by changes in bone shape: it has been suggested that early birth factors and activity at key stages of bone growth such as puberty may affect bone development (Figure 2). Other mechanical factors later in life, including heavy manual labour and joint damage that may contribute to abnormal hip shape, also significantly increase the risk of OA. Although not as strong a risk factor as for knee OA, obesity is also a risk factor for hip OA. However, in contrast to the knee, the evidence is that the effect is more mechanical than metabolic.7
{kind=link}
Hand osteoarthritis
Risk factors for hand OA include age, female sex and postmenopausal status.8 There is also evidence that obesity is a risk factor for hand OA, supporting the evidence that it is a metabolic mechanism underlying the disease.9
Features not to be missed
Features of OA not to be missed include:
- significant joint swelling/erythema (suggestive of inflammatory or crystal-associated arthritis)
- fevers (possible infection)
- significant neurological signs
- (e.g. with back or neck pain)
- other specific patterns suggesting a secondary cause of OA
- (e.g. isolated second and third metacarpophalangeal arthritis in haemochromatosis).
Initial investigations and tests
Establishing a diagnosis and patient education are key components of therapy and goal-setting in OA. A recent systematic review identified patient dissatisfaction related to a perceived lack of education and information about their OA.10
In most patients, a thorough clinical evaluation is sufficient for the diagnosis of OA.11 Investigations may be helpful to exclude other disease in the presence of atypical features including early morning stiffness (lasting more than 30 minutes), fevers, and joint swelling and erythema. Fibromyalgia and pain sensitisation syndromes also need to be considered in those with widespread pain.
Laboratory testing is usually only needed to exclude an alternative diagnosis or when the result of the investigation may alter the management (e.g. assessing renal function before taking an NSAID). Joint aspiration may be considered in the presence of a joint effusion where an alternative diagnosis such as septic arthritis or gout/pseudogout is suspected.
The role of radiographic investigations in OA is limited. However, plain radiographs may be required to exclude other joint diseases, occasionally validate patient concerns, and assess severity of the OA and the likely prognosis. For example, imaging may identify patients with end-stage knee OA and pain that does not settle with other treatments as suitable candidates for joint replacement.12
Although MRI has been proven to be very useful as a research tool that has enabled a greater understanding of the pathological processes in OA (especially in very early OA before any radiological changes are evident), its role in the clinic is extremely limited.13 Use in this setting can have unintended consequences: lesions that are part of the OA process may be identified and targeted even though there is no evidence that doing so will affect outcome. This has been clearly shown in the case of meniscal tears repaired with arthroscopy even though there is no evidence that this is more effective than physiotherapy and treatment may cause harm.14
Evidence-based treatments
GPs are central to the care of patients with OA, co-ordinating the multidisciplinary management with allied health practitioners and specialists, if required. The principles of OA management, as outlined by the RACGP and Australian Commission on Safety and Quality in Health Care guidelines, are:
- educating patients
- managing pain
- maximising function
- modifying risk factors (e.g. obesity and physical inactivity).12,15
Nonpharmacological management is almost always considered first-line treatment for patients with milder symptoms, particularly given that pharmacological treatments are associated with adverse effects. Common comorbidities including diabetes, cardiovascular disease and depression can be addressed when patients present with symptoms of OA.
Nonpharmacological treatments
The key components of nonpharmacological management of patients with OA are assessment, diagnosis, education and managing expectations. Treatment requires an individualised management plan and with ongoing review to monitor patients’ progress.12
Self-management education programs may provide clinical benefit by engaging a patient in goal-directed treatments. Weight loss, although difficult to achieve, is a key to improving pain and reducing disease progression.16,17 As there is a tendency for progressive weight gain with age, weight maintenance could be considered a more achievable alternative target.
The most effective therapy for OA, particularly knee OA, is exercise. A recent Cochrane review summarised evidence that any land-based exercise is effective in improving pain and physical function.18 Exercise will also help facilitate weight loss and improve muscle strength. Water-based exercises may be beneficial for patients with hip OA because land-based exercises are particularly painful.
Physiotherapy may be helpful in formulating a patient-specific approach to exercise, whereas occupational therapists may be helpful in providing strategies to overcome functional deficits.19 Devices such as splints, orthotics and braces may provide pain relief or improve function, particularly when the patient has mal-alignment or instability.19 Walking aids and appropriate footwear provide symptomatic relief while also reducing the risk of falls.19,20
Other nonpharmacological therapies that may provide symptomatic benefit include thermal agents (e.g. heat packs) and tai-chi programs.19,20 Acupuncture may provide small benefits for pain,21 but the use of transcutaneous electrical nerve stimulation is not supported by the literature.22 Fibromyalgia coexists in a significant number of patients with OA, and psychological interventions addressing central pain sensitisation such as cognitive behavioural therapy and mindfulness can provide benefit.23
Pharmacological treatments
Pharmacotherapy should be reserved for episodes of pain in OA and are mainly useful intermittently, particularly as the effect of most treatments is very small.24 Pharmacotherapy should be individualised, with particular consideration of patient comorbidities.12
Paracetamol is often the first-choice analgesic due to its favourable safety profile; however, there is some concern regarding toxicity even when used within the maximum dose of 4 g daily.25 There are no data suggesting added benefit of slow-release paracetamol.
NSAIDs have been shown to be more effective than paracetamol,26 but are associated with significant toxicity, particularly renal, cardiovascular and gastrointestinal. COX-2 inhibitors (e.g. celecoxib, meloxicam) are associated with slightly lower rates of gastrointestinal adverse effects, whereas naproxen may be associated with slightly lower rates of cardiovascular events.27 Topical NSAIDs have modest benefit,28 with a significantly more favourable adverse effect profile than oral NSAIDs.
Data regarding glucosamine remain conflicting with only glucosamine sulphate (not glucosamine hydrochloride) being shown to have small benefits on pain and function.29 There is some evidence of possible benefits with dietary supplements (e.g. Boswellia serrata extract, curcumin or pycnogenol) for pain reduction over the short term, but the quality of these studies is very low and so benefits and safety remain uncertain.30
Narcotic analgesia should be avoided given the limited efficacy and significant toxicity associated with its use.31
Intra-articular corticosteroids may be effective in improving pain and function, but only in the short term (e.g. one to two weeks).32 However, their use may provide the opportunity to institute other active treatments such as exercise. The evidence regarding intra-articular hyaluronic acid, platelet-rich plasma and stem cells are low quality and conflicting.33-35
Referral to a specialist
Referral of a patient may sometimes be required when the diagnosis is in doubt. Referral for joint replacement should be limited to patients with severe pain or functional limitation, who are not responsive to conservative or medical therapies, such as those at the later stages of disease.20 There is a limited role for joint arthroscopy given the small amount of data indicating benefit compared with the significant risk of adverse events:36 emerging data suggest these procedures may even result in accelerated joint damage.37
It is, however, important to note that even though joint replacement is effective, about 20% of patients having knee and hip replacements are dissatisfied with the results, even when the surgery is technically successful.38,39 Therefore, consideration of the timing of surgery is crucial. In the case of hip replacements, there is evidence that longer wait times for surgery result in deterioration in pain.40 However, there are emerging data that physiotherapy preoperatively can improve pain and quality of life.41
There is also evidence that for patients with end-stage knee OA it is possible to delay surgery using strategies such as weight loss.42 It may be that trialling other therapies before knee replacement and proceeding only when other therapies have failed will result in better patient outcomes, especially for knee joint replacements. Timing for joint replacement surgery is also important when considering that many prostheses will require revision surgery after several years.
Role of the GP
As the primary care provider, GPs provide the most important healthcare contact in providing and co-ordinating the care of patients with OA. Providing and monitoring evidence-based treatments, liaising with allied health professionals and referring patients for specialist evaluation for diagnostically uncertain or refractory disease are key aspects of a patient-centred approach to treating OA. GPs are also important in the postsurgical management of patients with OA.
Models of conservative OA care using a multidisciplinary team centred around a musculoskeletal co-ordinator (e.g. physiotherapists) have been developed – for example, the Osteoarthritis Clinical Care Pathway (OACCP) in New South Wales (https://www.aci.health.nsw.gov.au/resources/musculoskeletal/osteoarthritis_ chronic_care_program/osteoarthritis-chronic-care-program) and the Osteo arthritis Hip and Knee Service (OAHKS) in Victoria (https://www2.health.vic.gov.au/hospitals-and-health-services/patient-care/specialist-clinics/specialist-clinics-program/osteoarthritis-hip-knee-service).
Follow up
Exercise is a key component of pain management for OA and avoidance of physical inactivity is needed to maintain function and slow disease progression. Similarly, avoiding weight gain is crucial for reducing pain flares and disease progression where weight loss is not possible.
Regular reviews should be offered to patients with symptomatic OA that would include monitoring symptoms and function, efficacy of preventive and treatment strategies, and supporting self-management.12
When patients present with OA, it is a perfect opportunity to identify and manage cardiovascular risk factors. Those with knee OA have a fivefold increased risk of metabolic syndrome and high risk of death from cardiovascular disease. This is also the case for hip OA, but not with the same magnitude.
Some useful resources for patients are given in the Box.
{kind=link}
Future direction
Exciting developments are underway aimed at identifying new approaches to disease modification in OA, such as statins as potential disease-modifying agents and krill oil aimed at targeting joint inflammation. It is clear that the risk factors for OA differ across the joints, but the key to future research will be an increased understanding of the exact pathogenesis of OA. The clear message is that OA is not one disease, but rather a group of heterogeneous diseases. Even within a joint such as the knee or hand, the causes of OA differ. For example, about 30% of patients with knee OA and 20% of those with hand OA have evidence of low-level synovitis. Such findings mean that interventions aimed at targeting the pathological process can be tested, rather than a one-size-fits-all approach to the disease. It is hoped that these new, targeted approaches will help fill the major gap in disease-modifying therapies in OA.
Several clinical trials, including some currently registered on the Australian and New Zealand Clinical Trials Registry, are examining different types of stem cells in OA. However, most are early-stage phase 1 studies and although stem cells offer potential, it will be some time before their role in OA is clarified.
Conclusion
OA is a leading cause of pain and disability worldwide. Although OA is a heterogeneous group of diseases, there are many shared risk factors including obesity and advancing age. Management of patients with OA is largely centred around conservative measures with a focus on individualised, holistic treatment, incorporating physical activity and weight management. Patient engagement with a multidisciplinary team is important in optimising these key management principles, as the effect of weight management and exercise is as good, if not better than, pharmacotherapy. Future research into the pathophysiological changes across the affected joints will lead to targeted therapies. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.