Ocular allergies – a brief overview

Eye diseases
Allergy
Careful history taking can help differentiate ocular allergy from other forms of ocular inflammation. Simple first-line management options are usually sufficient for safe and successful management of most cases.
Ocular allergies are a common spectrum of disease processes that are usually mild, yet often annoying to the patient. Patients with an ocular allergy may present with a variety of symptoms including red, itchy and watery eyes. Careful history taking can help differentiate ocular allergy from other forms of ocular inflammation. Simple first-line management options are usually sufficient for safe and successful management of most cases. Complex cases that are refractory to first-line management options may require a multidisciplinary shared-care approach between the primary care physician and an ophthalmologist and, potentially, an immunologist.
Conjunctivitis is a common eye condition with numerous causes such as allergies, viral or bacterial infections, chemicals and dry eyes. Common symptoms include burning, scratchiness, itch, redness and watery eyes with a discharge.
Allergic conjunctivitis, in particular, is common and accounts for about 15% of all ophthalmic presentations in general practice. It is likely that the true incidence is underreported, as most patients with allergic rhinitis describe ocular symptoms when specifically asked about them.1 Allergic conjunctivitis is relatively benign; however, there are more severe causes of a red eye that need to be ruled out through careful history taking and examination. This can be a challenge, as specialist examination equipment such as slit lamps may not always be easily accessible in general practice.
Classification of ocular allergies
Ocular allergies are traditionally classified according to the underlying cause. The most common is allergic conjunctivitis, which may be acute, seasonal or perennial in nature.
Seasonal allergic conjunctivitis is usually self-limiting. Patients present with atopic symptoms such as lid swelling, pink or red eyes, sticky clear discharge and itch, which is a prominent symptom. Clinical examination of the patient’s eyes often reveals swollen lids, Dennie-Morgan infraorbital fold and dark circles,2 and pink oedematous conjunctiva with numerous small, flat-topped nodules with central vessels (papillae). Patients with perennial allergic conjunctivitis present in a clinically similar way to those with seasonal allergic conjunctivitis but usually have a milder clinical course and can present throughout the year. All types of allergic conjunctivitis are immunoglobulin E (IgE) mediated type I (immediate) or type IV (delayed) hypersensitivity reactions after exposure to an ocular allergen.
Other allergic conditions include:
- vernal keratoconjunctivitis
- atopic keratoconjunctivitis
- contact lens-associated papillary conjunctivitis (including giant papillary conjunctivitis)
- contact hypersensitivity (a form of lid or conjunctival delayed hypersensitivity due to cosmetics or ocular therapeutics)
- toxic follicular conjunctivitis (drug toxicity-related).
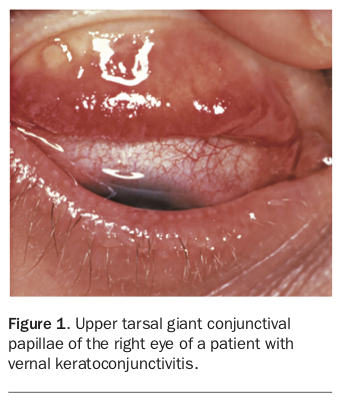
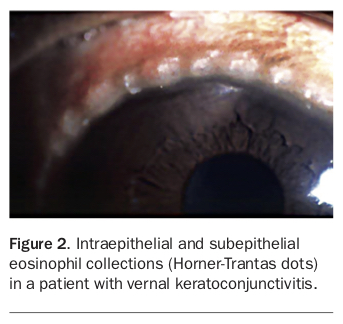
Vernal keratoconjunctivitis or ‘spring catarrh’ usually occurs in children. As the word ‘vernal’ suggests, symptoms are often worse in spring. Examination of the patient’s eyes reveals giant papillae in the tarsal conjunctiva (Figure 1), accompanied by thick, ropy, chewing-gum-like mucus and Horner-Trantas dots (Figure 2).
{kind=link}
{kind=link}
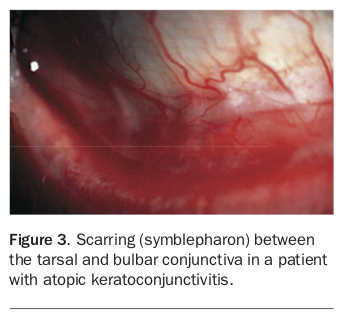
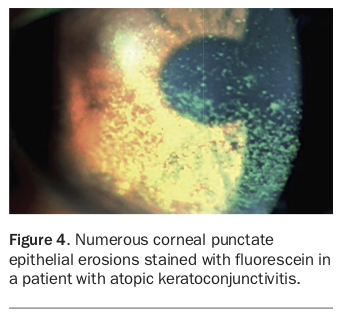
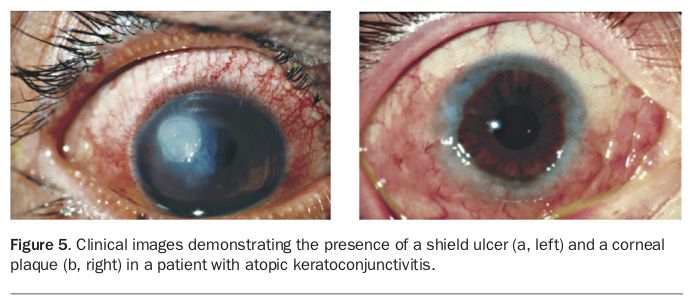
Patients with atopic keratoconjunctivitis tend to present in adulthood and with a watery discharge instead of the thick, ropy discharge present in vernal keratoconjunctivitis. It is associated with the presence of concurrent atopic diseases (e.g. atopic dermatitis). Examination shows changes in the eyelids (erythema, dryness, scaling or thickening) and conjunctiva (small papillae, scarring or adhesion [symblepharon] between the tarsal and bulbar conjunctiva (Figure 3) and Horner-Trantas dots), and corneal changes ranging from punctate epithelial erosions (Figure 4) to larger shield ulcers or plaques (Figure 5).
{kind=link}
{kind=link}
{kind=link}
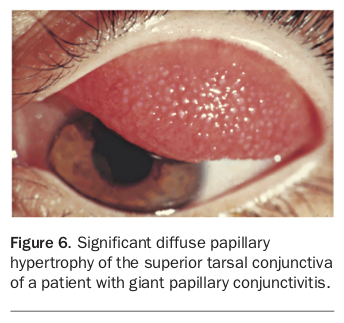
Giant papillary conjunctivitis occurs as a result of a foreign body reaction to contact lenses, prostheses or corneal sutures. Clinical signs include the presence of mucoid discharge and protein deposits on the contact lenses, and large papillae on the tarsal conjunctiva of the upper lid (Figure 6). Patients may also report that their contact lenses are excessively mobile. This is due to the upper lid capturing the contact lens.
{kind=link}
Toxic follicular conjunctivitis can be caused by almost any ophthalmic medication. Preservative ingredients in ophthalmic preparations that may trigger such an ocular allergy include thimerosal, chlorobutanol and benzalkonium chloride.3
Vernal keratoconjunctivitis or ‘spring catarrh’ is a type IV (delayed) hypersensitivity reaction. Atopic keratoconjunctivitis is a combination of type I and type IV hypersensitivity reactions. Similarly, giant papillary conjunctivitis is an immune response (type I and type IV) provoked by direct mechanical injury or contact with an allergen such as a contact lens (and/or other allergens coated on the ocular surface of the contact lens). Drug-induced toxicity can be IgE mediated, cell-mediated or a toxic reaction.
Assessment
Most commonly, patients with ocular allergies present with itchy eyes, oedematous conjunctiva and pink or red watery eyes, often with a sticky, clear discharge. A personal or family history of atopy is common. It is essential to ascertain whether the patient has experienced any loss of vision or has a history of dry eyes, contact lens use, self-administered topical eye drops, pre-existing ocular conditions (such as corneal abnormalities), or is taking any long-term oral or inhaled corticosteroids. These patients will benefit from management shared between the general practitioner and an ophthalmologist.4
Before commencement of any treatment, it is important to rule out infectious causes of conjunctivitis. Vision loss is generally minimal in cases of acute conjunctivitis but may occur with diseases that also involve the cornea, including viral keratoconjunctivitis and blepharoconjunctivitis, both of which are common presentations in primary care. Consider early referral of patients with perilimbal redness, intraocular pain, photophobia or vision loss, which are symptoms more typical of uveitis or corneal disease. Other important causes of a red eye include uveitis, angle closure glaucoma, episcleritis and scleritis.
Management
First-line conservative management of ocular allergies involves cool compresses, cold preservative-free artificial tears and careful identification and avoidance of triggering allergens. Pharmacological treatments include:
- dual-acting topical mast cell stabilisers/antihistamines, preferably in preservative-free formulations, can be used in adults and children 3 years or older. The two most commonly used formulations are:
– olopatadine 1 mg/mL eye drops, one to two drops in the affected eye(s) twice daily. Indicated for the treatment of the signs and symptoms of seasonal allergic conjunctivitis. Treatment may be maintained for up to 14 weeks, if considered necessary
– ketotifen fumarate 250 mcg/mL eye drops, one drop in the affected eye(s) twice daily. Indicated for symptomatic short-term treatment of seasonal allergic conjunctivitis - second-generation oral antihistamines (fexofenadine, loratadine, desloratadine, cetirizine), especially if systemic allergic symptoms are present
- topical NSAID
– ketorolac trometamol 5 mg/mL one drop [0.25 mg] instilled in the eye four times daily. Indicated for the short-term (2 to 4 weeks) relief of symptoms of seasonal allergic conjunctivitis - intranasal corticosteroids if symptoms of allergic rhinitis are present.5
If ocular allergies occur after administration of eye drops, preservative-free formulations can be obtained from most compounding chemists. Corticosteroid eye drops are usually reserved for patients in whom the disease is severe or refractory to other treatments. There is potentially an overlap of symptoms with dry eye syndrome and patients with recalcitrant symptoms should be managed with this in mind.
Given that patients with infectious keratitis or conjunctivitis can present similarly to patients with an allergic condition, it is paramount for all forms of infectious aetiology (bacterial, fungal, viral, protozoal) to be ruled out before commencing topical steroid eye drops. Corticosteroids can worsen the underlying disease process and it is best for GPs to avoid prescribing them in this setting. Patients should have a slit lamp examination to help rule out such opportunistic infections before being treated with corticosteroid eye drops. Patients who are prescribed corticosteroid eye drops may be at risk of drug-induced raised intraocular pressures and should be closely monitored by an ophthalmologist.
If the patient’s condition is recalcitrant to conservative treatment and topical corticosteroid use is not appropriate, the immunomodulator ciclosporin can be considered and administered in conjunction with an ophthalmologist. Cyclosporin 0.05% ophthalmic emulsion one drop twice daily is available through the PBS Special Access Scheme for severe dry eye syndrome. In patients with allergic polysensitisation or significant rhinoconjunctivitis, it may be worth considering allergen immunotherapy and desensitisation as an additional option that can be administered in conjunction with an immunologist.
Conclusion
Ocular allergies are common but often mild. Careful history taking can help discern ocular allergy from other forms of ocular inflammation. Although referral of patients with allergic conjunctivitis is generally nonurgent in nature, and may not be required for a straightforward case of simple allergic conjunctivitis, identifying red-flag symptoms is crucial for expedited referral and co-management between the general practitioner and a specialist. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.