Not good as new: how GPs can help cancer survivors live well after treatment

Cancer
Mental health
Follow up for people who have had cancer has shifted from a surveillance focus to an emphasis on living well using evidence-based treatment and co-ordinated and integrated care. Many aspects of assisting patients to live well after cancer can be provided by GPs.
Cancer is common, and the Australian Institute of Health and Welfare estimated that 134,174 new cases would be diagnosed in 2017.1 Improvements in early detection and treatment have led to increased survival, meaning that more people continue to live with the side effects of the cancer and its treatment. Survivorship has emerged as a key area in cancer care and GPs have a crucial role in supporting patients.
Emerging focus on survivorship
The diagnosis of cancer is distressing for the patient and their family and the initial phase of specialist review, investigations and making treatment decisions is challenging. Once a treatment plan is developed the person often feels that they can ‘get on with it’; however, treatments such as surgery, chemotherapy and radiotherapy may extend over many months. Emerging treatments such as immunotherapy can extend treatment even further, so that completion of treatment becomes less defined. Support will often be available from friends and family. Most people anticipate completion of treatment with a sense of relief and are dismayed to find that physical side effects persist (or even get worse, as in head and neck cancer) and the support received during treatment suddenly evaporates as others feel that the person should be getting back to normal. They might have survived, but they are not ‘good as new’.
How can GPs assist people to live well after cancer?
Until recently, follow up has tended to be surveillance based, with a focus on detection of recurrence and treatment of side effects. Cancer Australia’s principles of survivorship aim to centre care around the person affected by cancer, with an emphasis on living well using the best possible evidence and co-ordinated and integrated care.2 GPs can assist patients to live well after cancer by addressing various aspects of care.
Physical activity
The Clinical Oncology Society of Australia promotes exercise as an adjunct therapy that helps counteract adverse effects of cancer and cancer treatment.3 Being physically active and exercising regularly is important for the health, function, quality of life and possibly survival of people treated for cancer.3 GPs can:
- provide information about the benefits of exercise
- dispel myths and misperceptions about activity
- use motivational interviewing and supportive techniques to help initiate behaviour change
- offer referral to an exercise physiologist under the Medicare Chronic Disease Management - Individual Allied Health Services items. This is especially important for patients with complex comorbidities so that a safe, tailored exercise plan can be developed (for example, focusing on resistance training and building core strength and balance).
Fatigue
Fatigue is a common concern of patients during and after completing cancer treatment. Contributing factors can include side effects of treatment, anaemia, treatment with steroids and sleep disturbance. Inactivity contributes to deconditioning, which in turn compounds fatigue. Fatigue can be a marker for depression, so it is worth exploring mood and capacity for pleasure. Psychoeducation and cognitive approaches (e.g. challenging black-and-white thinking) in combination with physical activity are recommended.4 Increasing physical activity when you are tired is not an obvious thing to do, so the GP’s role is essential in providing information and guiding the person to initiate activity. More details are provided in the Facing the future section below and in the resources Box.
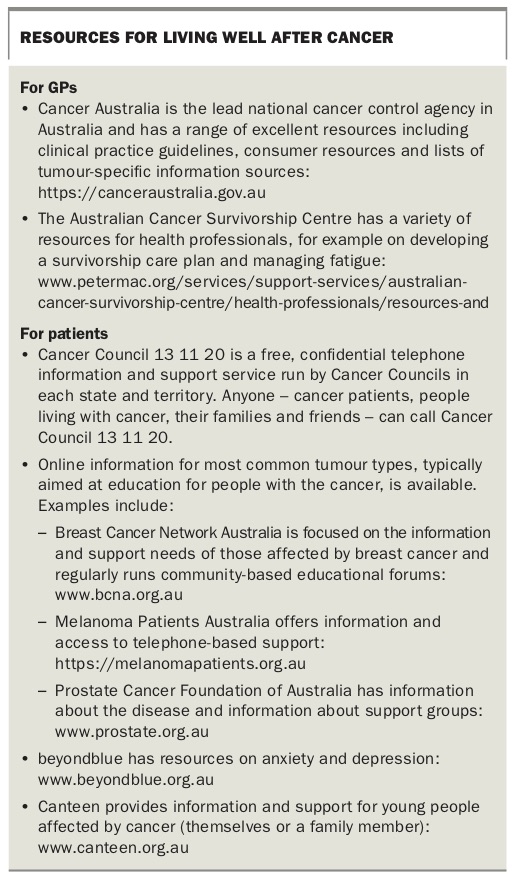{kind=link}
Nutrition and lifestyle
The WHO estimates that about one-third of deaths from cancer are due to five leading behavioural and dietary risk factors.5 GPs are well placed to use evidence-based techniques such as motivational interviewing to encourage behaviour change, especially in relation to smoking, alcohol use, fruit and vegetable intake and physical activity. Maintaining a healthy weight is important not only for general health but potentially to reduce the risk of cancer recurrence, and referral to a dietitian can be made using the Medicare Chronic Disease Management items.
Demystifying stress
It is natural to wonder why the cancer developed, and stress is commonly blamed. Any role played by stress is small and the National Cancer Institute and WHO state that there is no consistent evidence that stress causes cancer. GPs have a role in exploring patients’ beliefs about stress, including any pressure from well-meaning friends or family to ‘be positive to beat it’. Attempting to be positive poses an emotional burden – it is exhausting to try to contain frustration, anger or fear. Conversely, there is overwhelming evidence that being able to talk about feelings (even distressing ones like fear of dying) helps adjustment.6
Fear of recurrence
Concern that the cancer could come back (fear of recurrence) affects up to 70% of people treated for cancer, and for almost 40% of those this persists over many years.7 Fear of recurrence is often not proportional to actual risk and patients with low risk can have high fear of recurrence. The role of the GP is to:
- explore these concerns by asking the person questions (e.g. Do you worry your cancer may come back? How often do you think about recurrence? How much does this affect your quality of life?)
- acknowledge concerns rather than immediately offering reassurance, which does not help and inhibits the person’s ability to talk about their concerns
- explore the person’s desire for help (e.g. Would you like help to deal with your concerns about this?)
- avoid doing extra tests to try to help the person who is anxious – this conveys that there is some doubt in your mind and there is something about which the person should indeed worry.
Interventions based on metacognitive techniques, detached mindfulness and acceptance and commitment therapy are effective in reducing fear of recurrence.8 Most community-based psychologists have the necessary skills to deliver these techniques.
Depression and anxiety
Depression and anxiety are common in the general population and more so in those who have had cancer. The impact of depression in cancer care is particularly important. Depression reduces the ability to cope with the disease burden and the side effects of treatment and is associated with reduced adherence to medication recommendations.9,10 Even more concerning is evidence that severe depression has been directly associated with reduced cancer survival independent of medical variables, although the mechanism is unclear.11
GPs have a role in the treatment of depression using comprehensive evidence-based recommendations.12 An active approach to identifying a person’s risk of developing depression is helpful.
A past history of depression, social adversity, lack of support and a prominent symptom burden (e.g. related to lymphoedema) all increase the risk of depression. The term ‘financial toxicity’ is emerging to describe the financial strain imposed for many who have treatment for cancer. Out-of-pocket costs for surgical procedures or imaging largely contribute; however, paying for parking at a hospital, pharmaceuticals and aides also contribute to this burden. GPs should ask about financial strain as this is associated with a threefold increase in the risk of developing depression.13
Sexuality
Sexuality is easy to overlook but is an important part of wellbeing. Changes in body image, fatigue and chemotherapy-induced menopause are some of the many issues that impact on self-esteem and sexuality for people with cancer. Cancer Australia has a practical resource to assist GPs to initiate discussion.14 Although developed to address issues for women treated for breast cancer, many of the questions can be readily adapted to other patient populations.
Complementary and alternative therapies
It is important to ask if the person is using any treatments or therapies in addition to those that have been prescribed. GPs can explore details such as who recommends the therapies or treatments, the costs and what outcomes the person anticipates.15 Some therapies may be harmful and interact with medical treatments. For others there may be no evidence of benefit or harm. GPs have a crucial role in ensuring that patients have evidence-based information about any nonprescribed treatments they are taking. Patients can download a comprehensive information app developed by Memorial Sloan Kettering Cancer Centre.16
Facing the future
Having cancer reminds people that they are not bulletproof and commonly undermines confidence and optimism. For some people there may be a sense of ‘Why bother? Things always go wrong for me’.
Self-efficacy refers to the person’s belief in their ability to succeed at chosen tasks and achieve set goals, and is postulated to predict:
- whether the individual will initiate a response to challenges
- how hard they will work at those challenges
- the extent to which they will persist despite adversity or setbacks.17
GPs can promote self-efficacy by encouraging the individual to set realistic, defined and achievable goals (e.g. ‘I will walk the dog for 10 minutes each day’ compared with ‘I will be more active’). Mastery over small tasks leads to increased willingness to work on larger tasks. Research has shown that the impact of encouragement is more significant if the person doing the encouraging has status, prestige, trustworthiness, expertise and confidence.17 So a GP saying ‘I want you to give this a go. I really think you can do it’ can have a significant effect.
Conclusion
GPs have a central role in assisting patients to achieve optimal physical and psychological health after treatment for cancer. In addition to providing clinical guidance, GPs can direct patients to high-quality information. Evidence-based knowledge helps them to feel more in control and able to respond to the frequently-offered advice from friends and family members that may be idiosyncratic or clearly unhelpful. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.