Vaccination of immunosuppressed patients with autoimmune inflammatory rheumatic disease

Immunisation
Autoimmune diseases
Patients receiving immunosuppressive therapy for inflammatory arthritis are at high risk of infections that could be avoided by vaccination. But which vaccines can be safely administered to immuno suppressed patients and which should not be used in this population?
Patients with autoimmune inflammatory rheumatic diseases (AIIRDs), such as rheumatoid arthritis, psoriatic arthritis and spondyloarthritis, often experience infections that could be prevented or attenuated by appropriate vaccination. However, vaccination might not be administered because of physician uncertainty about timing and which patients with AIIRDs should be vaccinated. There is also concern about the use of live vaccines in patients with immunosuppression.
Immunosuppression and vaccines
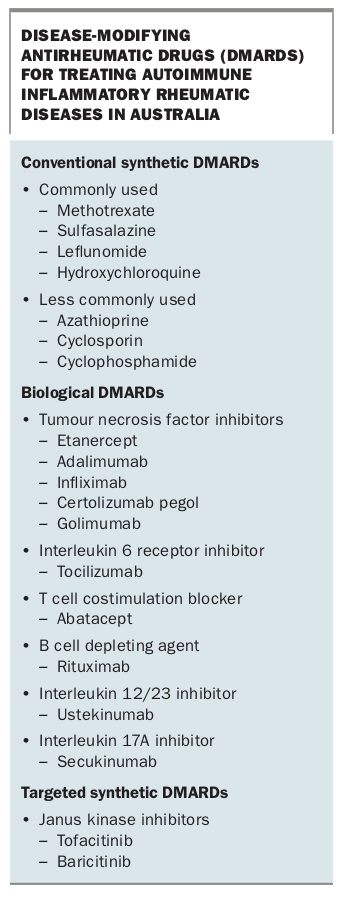
Immunosuppressive therapies to treat AIIRD include corticosteroids and conventional synthetic disease-modifying antirheumatic drugs (DMARDs), such as methotrexate, sulfasalazine, leflunomide and azathioprine (Box). The treatment of AIIRD has been revolutionised by the widespread use of biological DMARDs, such as etanercept and rituximab, which target proinflammatory cytokines and cell types, respectively, and, more recently, novel targeted synthetic DMARDs, such as tofacitinib and baricitinib, which target specific proinflammatory enzymes (Box).
{kind=link}
Live vaccines are generally contraindicated in severely immunocompromised patients because of the possibility of vaccine-induced disease from uncontrolled in vivo viral replication.1 Use of high-dose corticosteroids (more than 20 mg daily of prednisone or equivalent) for more than 14 days or treatment with a biological DMARD is thought to contraindicate live vaccine administration.1,2 However, low-dose corticosteroids (equivalent to less than 20 mg daily of prednisone), or the usual doses of methotrexate (less than 0.4 mg/kg per week) and sulfasalazine or azathioprine (less than 3 mg/kg daily) that are used to treat AIIRD, are regarded as low-level immunosuppression and may not contraindicate administration of some live vaccines, such as the herpes zoster (HZ) vaccine.
Although this is a broad area, the following cases represent common clinical scenarios.
Case 1: Herpes zoster vaccine
Mrs Smith is a 72-year-old woman who is taking methotrexate (20 mg per week) for rheumatoid arthritis. She has heard that she’s eligible for the ‘shingles vaccine’ on the ‘free list’ but wonders whether it’s safe for her to receive this vaccine while taking methotrexate.
Commentary
The incidence of HZ, or shingles, in people aged 50 years or older in Australia is about one in 100, with an increased risk in the elderly and patients with AIIRD receiving immunosuppressive therapy.3 The complications of postherpetic neuralgia and HZ ophthalmicus result in significant morbidity.
The live attenuated HZ vaccine functions as a booster and is used to prevent shingles in those with (or presumed to have had) previous varicella-zoster virus (VZV) exposure. The Australian National Immunisation Program (NIP) recommends the live attenuated HZ vaccine for people aged 70 years, with a catch-up program for those aged 71 to 79 years.1 Mrs Smith is therefore correct; she qualifies for free vaccination with this vaccine under the NIP.
In contrast to the HZ vaccine, the varicella vaccine contains a lower dose of live attenuated Oka varicella virus and is used to prevent chickenpox in those lacking VZV immunity. Although there is usually no need to check VZV immunity status before vaccination in healthy patients, it is wise to do this in immunocompromised patients, such as Mrs Smith. If there is no serological evidence of previous VZV exposure, vaccination with the varicella vaccine to prevent chickenpox should be considered (two doses separated by at least four weeks in those aged 14 years or older).1
As the dose of methotrexate Mrs Smith is taking to treat her inflammatory arthritis represents low-level immunosuppression, it is not a contraindication to the live attenuated HZ vaccine. So, she does not need to stop taking methotrexate before receiving this vaccine.1,4,5 However, she should seek urgent medical attention if she develops a viral illness or vesicular rash after receiving the vaccine.
Mrs Smith’s regimen is changed to methotrexate (20 mg per week) and the tumour necrosis factor (TNF) inhibitor adalimumab (Humira 40 mg subcutaneously every two weeks). Is she still able to receive the live attenuated HZ vaccine?
Commentary
All patients aged 50 to 80 years should be considered for HZ vaccination before starting treatment with a targeted synthetic DMARD or biological DMARD, such as adalimumab. (Those aged under 70 years will not receive free HZ vaccination under the NIP, and the cost for a private prescription is about $200.) Although data are lacking, some guidelines suggest a biological DMARD needs to be stopped from one to 12 months before administration of a live vaccine.1,6 However, this wide range is unhelpful and impractical in many patients with severe inflammatory arthritis, as their arthritis often flares after delaying or missing even one dose of a biological DMARD.
On closer questioning, although Mrs Smith’s rheumatoid arthritis is now well controlled, her joint symptoms flare if she misses or is late with a dose of Humira. After discussing the possible but low risk of HZ infection from the live attenuated HZ vaccine, Mrs Smith’s rheumatologist advises her to miss one dose of Humira before receiving this vaccination, have the vaccination on the day of the missed dose and recommence Humira two weeks later. Mrs Smith is advised to seek urgent medical attention for prompt antiviral therapy if she develops a viral illness or vesicular rash after receiving the live attenuated HZ vaccine.
As this is a complex area, seeking expert opinion from the treating rheumatologist when considering HZ vaccination in patients being treated with biological or targeted synthetic DMARDs is recommended.
Additional information
There is a new recombinant HZ vaccine that has greater efficacy than the live attenuated HZ vaccine and provides immunity that does not seem to wane with age.5,7 The recombinant HZ vaccine has been approved for use in Europe, Canada and the US. Although use of a recombinant preparation means there is no risk of generalised VZV infection after vaccination, long-term follow up of immunosuppressed patients who received this vaccine is limited.
In November 2018, the Australian Pharmaceutical Benefits Advisory Committee did not recommend listing the recombinant HZ vaccine on the NIP for preventing HZ in adults aged 60 years or older, largely because of cost considerations. However, a future regulatory submission for recombinant HZ vaccination in immunocompromised people is likely.
Case 2: Influenza vaccine
Mr Tan is a 65-year-old man taking prednisone (5 mg daily) and methotrexate (20 mg per week) for psoriatic arthritis. It’s autumn, and he wonders whether he should get the ‘flu shot’.
Commentary
Immunosuppression is associated with an increased risk of influenza-related complications. As influenza vaccination is the most important intervention for preventing or attenuating infection and reducing hospitalisation and mortality,8 Mr Tan should definitely receive it.
Quadrivalent influenza (inactivated virus) vaccines are recommended for people aged from 6 months to less than 65 years of age.1 Quadrivalent vaccines are preferred over trivalent vaccines because they may offer a greater range of protection. However, two different trivalent (inactivated virus) vaccines – a high-dose trivalent vaccine and a trivalent vaccine with a potent adjuvant to boost immune responses – are recommended for people aged 65 years or older, such as Mr Tan, due to age-related waning immunity.1
Although a lower seroprotective response may be seen in the presence of DMARDs, most patients have an adequate level of protective antibody after influenza vaccination, with no worsening of AIIRD symptoms.9,10 The exception to this is in patients taking rituximab, which causes prolonged B cell depletion for six to 12 months. As this prevents the development of an effective postvaccination protective serological response, vaccination needs to occur before administration of rituximab.
Immunocompromised patients with AIIRD should receive the influenza vaccine annually before the start of the influenza season, as protection is greatest in the first four months after vaccination. There is some evidence that patients with AIIRD who receive the influenza vaccine for the first time should receive two doses at least four weeks apart, and one dose annually thereafter.11
Case 3: Pneumococcal vaccine
Mr Jones is a 65-year-old man with rheumatoid arthritis that is managed with methotrexate (15 mg per week) and sulfasalazine (1 g twice daily). He has a history of chronic obstructive pulmonary disease but stopped smoking 10 years ago. His GP wonders whether he should be given the pneumococcal vaccine.
Commentary
Invasive pneumococcal disease, such as pneumonia, often occurs in immunosuppressed patients. As Mr Jones has underlying lung disease from smoking and is immunocompromised, he is at significant risk of infection. He should definitely receive pneumococcal vaccination.
There are two pneumococcal vaccines available:
- 13-valent pneumococcal conjugate vaccine (13vPCV)
- 23-valent pneumococcal polysaccharide vaccine (23vPPV).
Mr Jones’ immunosuppression places him in the highest risk category for invasive pneumococcal disease, and he has never previously been vaccinated. He should therefore receive the 13vPCV, before receiving the 23vPPV two months later, as a ‘prime and boost’ strategy to provide broader protection.1 An additional dose of 23vPPV can be given five years later.
As there is some attenuation of postvaccination serological response in patients taking methotrexate, it is ideal to administer the vaccination before starting DMARDs, but this is not always practical.
Case 4: Infant vaccinations
Ms Wilson is a pregnant 34-year-old woman being treated with intravenous infliximab (Remicade) for ankylosing spondylitis. She has elected to continue Remicade treatment throughout pregnancy because the ankylosing spondylitis previously made her life a misery. She wonders whether Remicade will cause any problems with her new baby’s vaccination program.
Commentary
Use of a monoclonal TNF inhibitor antibody during pregnancy raises concern for the newborn infant, as monoclonal antibodies such as infliximab or adalimumab (Box), which are immunoglobulin (Ig) G1 molecules, are actively transported across the placenta to the fetus from 16 weeks of gestation. Although this allows transfer of protective passive immunisation (maternal antibody) for the first 6 months of life, it also means the newborn may be immunosuppressed, as active transport of infliximab results in levels in the newborn that exceed maternal serum levels. This has implications for a live vaccine given to the infant in the first 12 months of life.
The only live vaccine listed on the NIP for administration in the first 12 months is the rotavirus vaccine, which is given at 2 and 4 months of age, or 2, 4 and 6 months, depending on the preparation.1 Ms Wilson should be advised to avoid rotavirus vaccination for her new baby, as there is a small risk of rotavirus infection from the vaccine. The likelihood of rotavirus infection is lower in infants older than 6 months, so if the vaccine is omitted, a catch-up dose may not be necessary. As rotavirus vaccination is part of the NIP, an unvaccinated infant may be protected by herd immunity.
All other NIP vaccinations in the first 12 months of life are safe in this context. The other live vaccines for infants (measles-mumps-rubella and varicella) are recommended for children aged at least 12 months and can be safely given even if the mother is breastfeeding, as transfer via breast milk is minimal.
Additional information
Certolizumab pegol, a TNF inhibitor, lacks a fragment crystallisable portion and so does not cross the placenta, nor does it appear to enter breast milk.12,13 Live vaccines can be given to infants born to mothers who were treated with certolizumab pegol during pregnancy.
Other vaccines
Diphtheria, tetanus and pertussis
Adults aged 50 years or older who have not had a booster dose of diphtheria and tetanus toxoids vaccine in the preceding 10 years should receive the dTpa vaccine (diphtheria-tetanus-acellular pertussis vaccine, reduced antigen content formulation). Note that this formulation differs from DTPa, which is used for children.1
Measles, mumps and rubella
As the measles-mumps-rubella vaccine is a live virus preparation, it is not recommended for use in immunosuppressed patients. Postexposure prophylaxis for nonimmune adults exposed to measles or rubella (but not mumps) should comprise normal human immunoglobulin administered within three days of exposure.1
Vaccination for travellers with AIIRD
This is a complex area that has recently been discussed elsewhere.6,14
Conclusion
The vaccination status of patients with AIIRD should be regularly reviewed as a collaboration between the patient’s GP and rheumatologist and, if required, an infectious disease physician. Although vaccination should occur before starting immunosuppressive therapy, for practical reasons this is usually difficult. Planning for overseas travel or pregnancy is an opportune time to review a patient’s vaccination status. MT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.