Eating disorders: the pivotal role of GPs

Eating disorders
Mental health
GPs arguably play the most important role in the management of eating disorders. They are often the point of first presentation, have a broad ongoing relationship with the person and vital medical skills.
With a new suite of 40 psychological and 20 dietetic sessions for people with eating disorders – that can all be accessed by general practitioners – introduced on 1 November 2019 under the MBS, the GP’s role in the management of this patient group is only set to grow. (For more information on the changes visit www.mbsonline.gov.au/internet/mbsonline/publishing.nsf/Content/Factsheet-EatingDisorders).
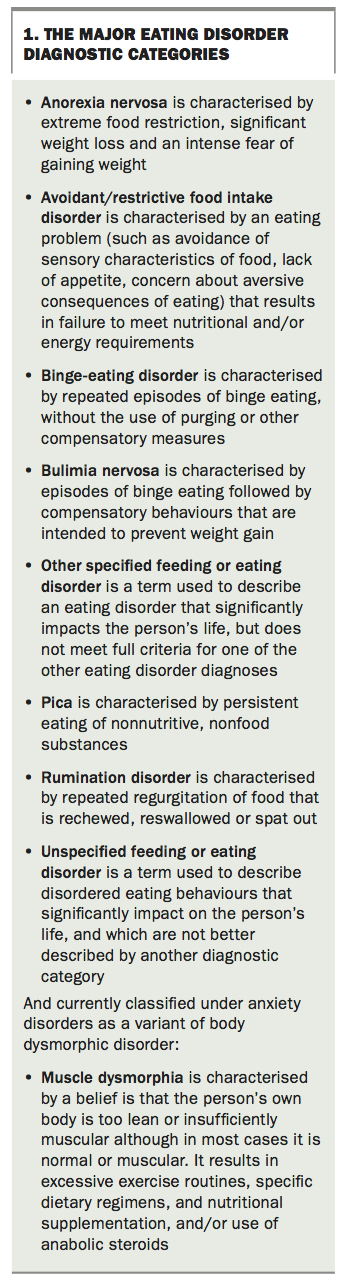
The term eating disorders describes a group of illnesses including anorexia nervosa (AN), bulimia nervosa (BN), binge-eating disorder (BED) and other feeding and eating disorders of childhood and adulthood. Box 1 summarises the major eating disorder diagnoses. They are defined by changes in behaviours, thoughts and attitudes to food, eating, weight or body shape that interfere with and detrimentally impact on a person’s life.
{kind=link}
Eating disorders are often comorbid with other mental health concerns, such as depression and anxiety. Observable symptoms of an eating disorder may be minimal or absent despite a person experiencing profound inner turmoil. Eating disorders are often all-encompassing, and affect a person’s body, feelings, thoughts, and behaviours in multiple ways. As a GP is likely to be one of the first health professionals with whom a person with an eating disorder will come in contact, and perhaps the only health professional who will have an ongoing relationship with the person over time, the GP’s role is pivotal and includes prevention, identification, medical management and referral.
Disordered eating
Not all disordered eating behaviours meet the criteria for a diagnosis of an eating disorder. Disordered eating can take many forms, including binge eating (eating an unusually large amount of food while feeling a loss of control), purging (by inducing vomiting) and engaging in other compensatory behaviours such as diuretic or laxative use. It also includes severely restricting intake in an effort to lose weight, engaging in excessive exercise, chewing and spitting food, fasting and yo-yo dieting.
Disordered eating alone confers poorer health outcomes in adolescence and into adulthood and so should be regarded as an important health index. Several studies have examined eating disorders and disordered eating longitudinally in adolescence and their relationship to longer-term health outcomes.
Adolescents with disordered eating behaviours (as well as those with eating disorders) have a substantially elevated risk for a range of health problems in adulthood including full-blown eating disorders, anxiety disorders, cardiovascular disorders, chronic fatigue and chronic pain syndromes, depressive disorders, suicide attempts and an elevated risk for being overweight or obese.1-6
Screening for eating disorders
Asking about dietary habits needs to be a routine part of care in general practice, given the importance dietary habits have in many physical and mental health conditions. The prevalence in the general population of eating disorders is about 5% at any one time. High prevalence and the serious long-term health implications of disordered eating suggest that formal screening for disordered eating and eating disorders in high risk groups should form a routine part of practice.
There are a number of groups within the community that have been shown to be at significantly higher risk of developing an eating disorder (Box 2).
{kind=link}
The SCOFF questionnaire is a five- question screening tool designed to screen for the presence of an eating disorder:7
S Do you make yourself sick because you feel uncomfortably full?
C Do you worry you have lost control over how much you eat?
O Have you recently lost more than one stone (6.35 kg) in a three-month period?
F Do you believe yourself to be fat when others say you are too thin?
F Would you say food dominates your life?
A ‘yes’ response to two or more of the five questions warrants further questioning and more comprehensive assessment by a healthcare professional.
Using the SCOFF questionnaire will help identify patients with eating disorders, but a dietary history should still be taken to ascertain whether subsyndromal disordered eating is present and likely to become a problem in the future.
Signs and symptoms
GPs are in a unique position to monitor a patient’s relationship with their body shape and weight and food because of the ongoing nature of the GP–patient relationship.
Research suggests there is an average delay of four or more years between the start of disordered eating and first treatment, hence the importance of the primary practitioner in being alert to signs and screening appropriately.
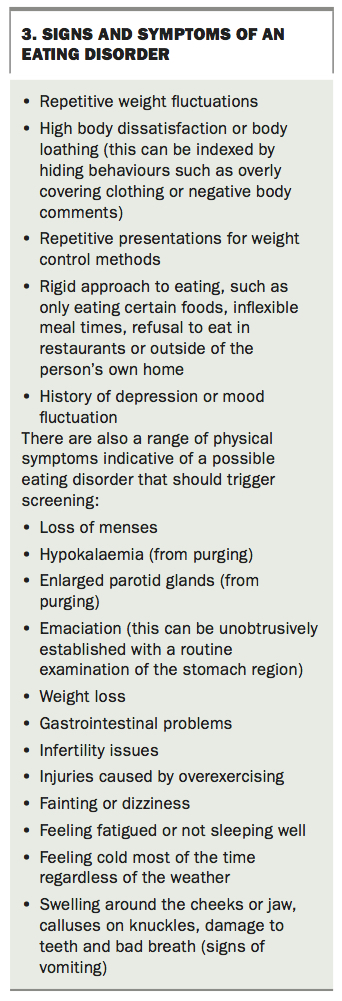
Even in the absence of a formal assessment there are markers that should alert the GP to the possibility of an eating disorder, and trigger a screening. These signs and symptoms are summarised in Box 3.
{kind=link}
Differential diagnosis and testing
It is important to exclude physical illness when weight change as a result of disordered eating behaviours is observed. Diagnoses can easily be missed if an assumption is made that the problem is an eating disorder. Many physical conditions are associated with weight and appetite changes.
An initial consultation for eating-related issues needs to include two categories of investigations: the first to exclude underlying physical conditions; and the second to determine whether the disordered eating has impacted on the patient’s physical state.
These investigations should include a full blood examination, liver, renal and thyroid function tests and any other investigations that may be appropriate depending on the patient’s symptoms. Diabetes, thyroid disease, haematological or other malignancies, inflammatory bowel disease, severe dental problems, gastric reflux and many other conditions are included in this list.
The clinician must investigate judiciously based on the clinical presentation. In some instances, the diagnosis may well be so clear that nothing beyond the basic tests will be required.
What causes eating disorders?
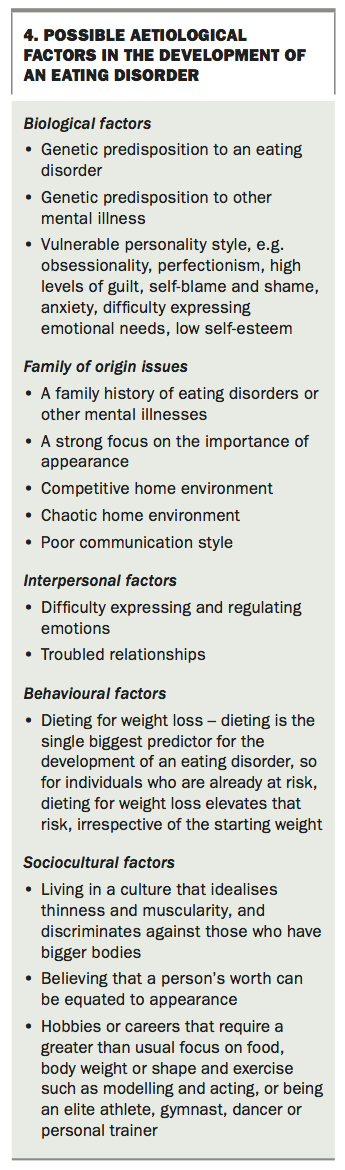
Box 4 lists the many possible aetiological factors in the development of an eating disorder. For most people, a number of factors can be identified as important in the initiation and maintenance of the disorder. Dieting for weight loss is the single most potent predictor of the onset of an eating disorder but not everyone who diets develops an eating disorder so other vulnerabilities may play a role.1,5,6 When encouraging obese and overweight patients to diet for weight loss, the risk of developing an eating disorder if other factors are present needs to be taken into consideration and weight loss approached with care.
{kind=link}
Role of the GP in treatment
Assembling and co-ordinating the treatment team
Because these illnesses affect both psychological and physical health, the treatment of established eating disorders requires a multidisciplinary team. Essential to the team are a GP to monitor the patient’s physical health, a therapist to provide focused psychological interventions for both the eating disorder and any underlying or comorbid psychological conditions, and a dietitian. The lines of communication between these practitioners need to remain open at all times and their roles should be clearly defined. Issues such as the frequency of medical visits, determining who is responsible for weighing the patient and communicating that information to other team members, and how nonadherence to treatment regimens should be managed need to be agreed on early. The patient’s GP is ideally placed to co-ordinate these various aspects of care.
Other practitioners who may need to be part of the treatment team include an endocrinologist, a gynaecologist, a paediatrician, a gastroenterologist, a dentist, a psychiatrist, a social worker and others, depending on the issues that arise in the course of the illness.
Medical monitoring
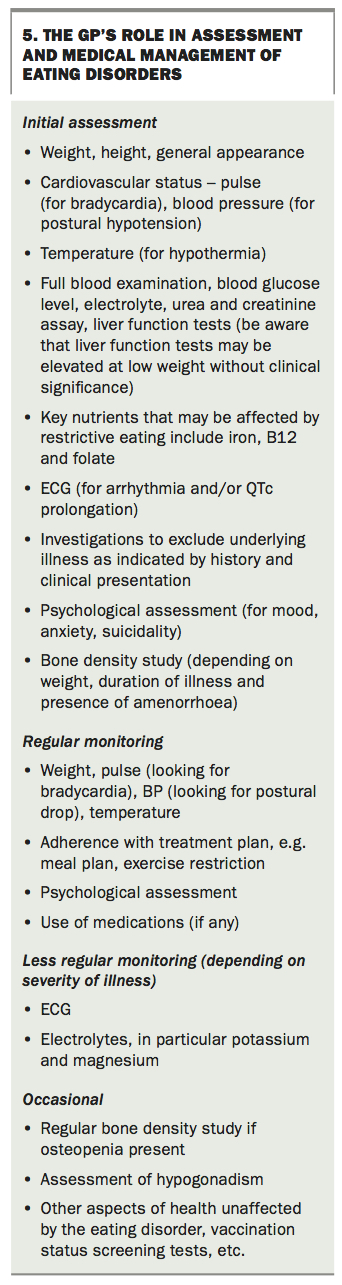
Careful consideration needs to be given to the frequency of medical monitoring as determined by the severity of the disorder and the impact of the illness on the patient’s physical health. At minimum, patients need to be weighed and have their cardiovascular status assessed (pulse rate and postural hypotension) regularly. For patients who are seriously underweight or who are purging frequently, especially those who are underweight and also purging, this will be at least fortnightly. These patients will also need regular blood tests to check for electrolyte disturbances and monitoring of their ECG, looking for QTc wave prolongation. In view of the risk of hypothermia in severely ill patients, monitoring body temperature is also important. Less frequently, patients will need monitoring for osteoporosis and other long-term complications of their disorder. A referral to hospital may be needed if medical stability cannot be achieved or sustained. Box 5 summarises the GP’s role in assessment and medical management of eating disorders.
{kind=link}
Psychological support
Regular medical monitoring provides the GP with the opportunity to maintain a relationship with the patient with an eating disorder and acknowledge them as a whole person not just a person with an eating disorder. This can be a very important aspect of therapy. It also provides the patient with another person who has an eye on their psychological wellbeing and allows psychological deterioration or suicidality to be identified early. GPs need to have that aspect of their role in mind when seeing patients with eating disorders and take the opportunity to get to know the person behind the illness.
Shame and stigma
A key deterrent to early identification and intervention is the shame and stigma felt by the patient. Most people with an eating disorder experience shame about their illness – binge-eating and purging behaviours are particularly shame-inducing. GPs should always use a nonjudgemental stance when asking about these behaviours and, whenever possible, reduce shame and normalise these behaviours as an expected feature of an eating disorder presentation.
Externalising the illness from the person, a strategy adopted from narrative therapy, is a useful approach to adopt in all situations involving dealing with a person with an eating disorder.8 The purpose of externalising is to convey to the patient and their carers that the person is not the problem and they have nothing to be ashamed of, and it is the eating disorder that is the problem (Box 6).
{kind=link}
Eating disorders can be experienced by the person as helping them to function by numbing their emotions, providing a distraction or sense of accomplishment, helping them to feel in control, and forming a part of a their identity. Understanding and validating that this is what the eating disorder does for them is often the key to successful engagement, and to reducing shame. However, sometimes people with a chronic course of illness do not respond well to externalisation of the illness. So if a patient reacts negatively to this technique you should stop using it.
Motivation and ambivalence
A core symptom of an eating disorder presentation is ambivalence, which usually presents as fluctuating feelings and thoughts about needing or wanting help, or indeed about anything actually being wrong. Motivational enhancement therapies emphasise accepting this as part of the presentation, rather than trying to eliminate or tackle it head-on. The essence of working with a person with fluctuating motivation is respecting that it is they who must find the solution, with the practitioner acting in a supportive and facilitating role. In practical terms, this may involve acknowledging and validating the person’s feelings about change, asking them what they would like help with, working with them on these aspects, and linking change to the person’s goals rather than the practitioner’s goals for them.
The RULE of thumb is a guide to motivational work:
Safety
Patients with eating disorders must be screened for physical and mental health risks. Medical stabilisation, when required, must be provided before or with other interventions. Eating disorders can impair a person’s insight and ability to make informed decisions. Decisions regarding treatment must always take into consideration the person’s capacity to make decisions for their own safety. People with eating disorders have high rates of suicide attempt and completion so risk assessment should always be undertaken. Box 7 provides a list of patient resources.
{kind=link}
Work collaboratively with patients and their families
Whenever possible, involve families and carers in the treatment process, providing information, education and support for the patient and their family. Including the patient’s family in assessment, treatment and recovery support is effective.
Conclusion
GPs play a vital role in the management of people with eating disorders. They are best placed to be the health professional who first identifies the presence of illness and usually the only health professional with an ongoing relationship with the patient (and often their family). GPs are often pivotal in establishing the multidisciplinary team necessary in the treatment of eating disorders. They can play a unique role in seeing the person as a whole, supporting them and the family through treatment and providing continuous monitoring and case management guidance. MT
Dr Orman: None.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.