Dealing with depression and medical illness

Depression
Mental health
Many physical illnesses are associated with depression, and GPs regularly encounter people with medical illnesses who also have depression. GPs can efficiently and effectively lead the management of these patients.
- GPs can conduct efficient and effective assessments of depressive symptoms in people with medical illnesses in primary care settings.
- Depression can exacerbate symptoms of medical illnesses and medical illness can exacerbate depressive symptoms.
- Some commonly used medications for conditions such as heart disease, airways disease and cancer are associated with symptoms of depression.
- GPs are best placed to manage care for most individuals with depression, but should always refer to a psychiatrist when in doubt.
Depression profoundly affects the presentation and management of medical illness. It reduces patients’ adherence to medical treatment and their quality of life, and increases rates of hospitalisation and mortality.1 Recognition and appropriate management of the depression is key but can be challenging. The overlap between symptoms of depression and many physical illnesses can complicate the diagnosis, and treatment for one condition can sometimes exacerbate the other.
Despite these issues, efficient assessment and treatment of depression in people with medical illnesses is achievable in general practice. The GP often has a rapport with the patient and the knowledge of their psychological, social and cultural history that is integral to managing the illness. Although the assessment process and treatment plan will depend on each patient’s unique presentation, there are a number of elements common to effective management for patients with medical illness and depressive symptoms.
Why is depression more common in people with medical illness?
The relation between depression and medical illness is complex (Figure). Biological factors contribute to the development of depressive symptoms in people with medical illnesses, but their relative contribution varies and is difficult to quantify. The effects of chronic inflammation, changes in the parasympathetic and sympathetic nervous systems and disturbances in the hypothalamo-pituitary axis are all considered relevant.2 Abnormalities such as high concentrations of proinflammatory cytokines have been noted in studies of people with depressive symptoms, but there is considerable heterogeneity in the literature.3,4
{kind=link}
Similarly important, yet difficult to quantify, is the role of sociological factors in the development of depressive symptoms in individuals who are medically ill. Childhood adversity and poverty predispose people to develop both depression and many medical illnesses.5 Adverse health behaviours, including smoking, poor diet and a sedentary lifestyle, are associated with these negative sociological factors and also predispose to depression and medical illness. The impact of chronic medical illnesses on a person’s lifestyle must also be considered. Practical effects on independence, employment and familial roles can be problematic, as well as the psychological effects on a person’s sense of self and, in some cases, a confrontation with one’s own mortality, in the face of diagnosis of a medical illness.6
Although it is difficult to quantify the contribution of different risk factors in the development of depression in people with medical illness, it is useful to consider possible biological, psychological and social contributors. This can be particularly helpful for taking a targeted history of an individual with a medical illness who presents with depressive symptoms.
Diagnosis
History
History taking should cover the possible psychological, social and cultural aspects of living with a medical illness. This provides an understanding of the contributing factors to the patient’s depressive symptoms and might also give some clues to appropriate treatment recommendations for each patient. It is the first step towards a tailored management plan for the person with medical illness and depression.
Diagnostic manuals, such as the DSM-5 (Diagnostic and statistical manual of mental disorders) and the ICD-10 (International statistical classification of diseases and related health problems 10th revision), contain diagnostic criteria for major depressive disorder. The criteria in these manuals are similar. However, these criteria pose difficulties when assessing depressive symptoms in someone with medical illness due to the overlap of physical symptoms between those of depression and many physical illnesses. Symptoms such as sleep disturbance, weight loss or impaired concentration are often present in renal disease, endocrine disorders and many malignancies.
The difficulties of diagnosing depression in people with medical illness have long been recognised. A number of screening tools have been devised to deal with this problem, which generally focus on the cognitive symptoms of depression. For example, the Beck Depression Inventory for Primary Care is a seven-item screening instrument that focuses on sadness, pessimism, past failure, loss of pleasure, self-dislike, self-criticalness, and suicidal thoughts or wishes. This tool is relatively brief and its sensitivity is comparable to other screening tools, such as the Hospital Anxiety and Depression Scale and the Patient Health Questionnaire that have been used for identifying depression in people with medical illnesses.7
Symptom rating scales should not be used simply to ‘add up’ symptoms. The duration of any symptoms of depression and the associated functional impairment must also be considered. Furthermore, none of these tools is a substitute for a thorough mental state examination that factors in the patient’s unique social and cultural factors.
Examination
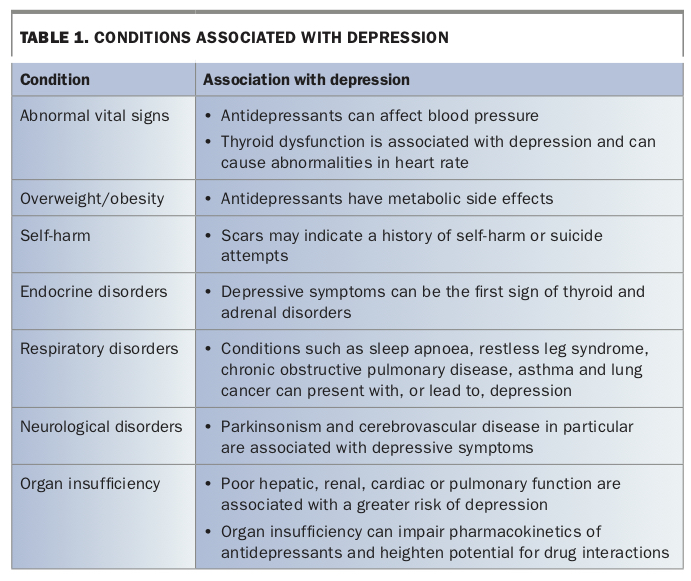
A comprehensive physical examination is crucial when assessing depressive symptoms in anyone with a medical illness. Depressive symptoms may signal an exacerbation of the original illness or be an early sign of another physical illness (Table 1).
{kind=link}
Particular attention should be paid to any evidence of endocrine disorders such as thyroid or adrenal disease, respiratory disorders such as obstructive sleep apnoea or chronic obstructive airways disease, or neurological disorders such as Parkinson’s disease and cerebrovascular disease.8-11 These diseases are not just associated with major depressive disorder; depressive symptoms can also be a feature of the illness itself.
Many psychotropic medications are associated with weight gain and metabolic disorders. Physical signs of metabolic syndrome should be noted. At minimum, this should include assessment of body mass index and waist circumference. Baseline measurements can assist in formulating a management plan for these issues.
Investigations
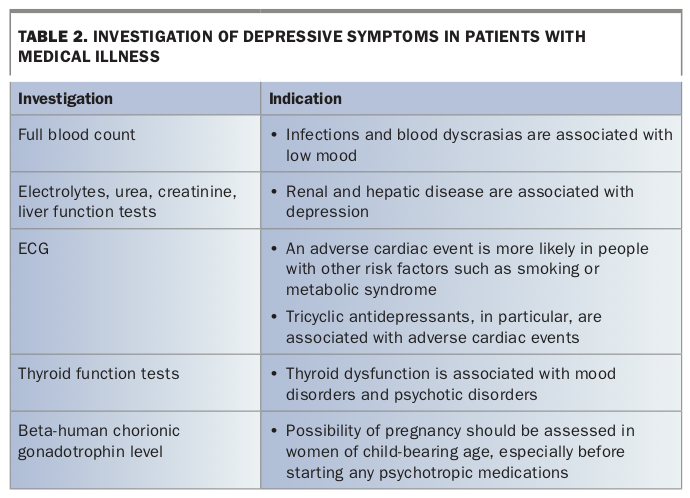
Clinically appropriate investigations should be carried out on an individual basis and baseline investigations conducted before starting psychotropic medications. A useful but not exhaustive guide to investigation of depressive symptoms in individuals with a medical illness appears in Table 2. People with unusual or treatment-resistant depressive symptoms may require specialist referral, further imaging, or even genotyping or pharmacogenetic testing.12
{kind=link}
Depending on the history and physical examination, inflammatory markers and microbial serology may be indicated. Infection with viruses such as varicella zoster, Epstein-Barr and herpes simplex type 1 or bacteria such as Chlamydia trachomatis is associated with increased rates of depression, but people with these infections rarely present with depression as a first symptom. In some patients, it may also be relevant to measure vitamin levels, as guided by the history and examination, because deficiencies of vitamin B12, vitamin B6, folate and vitamin D are associated with depression.
Management
Successful treatment of depression in someone with a medical illness depends not only on making the correct diagnosis, but also on gauging the severity of the depression. Mild-to-moderate depressive episodes may be adequately managed with psychological interventions alone, but patients with severe depression may also benefit from medications or other nonpharmacological strategies.
Standard interventions
General measures can significantly reduce depressive symptoms and should always be implemented even in cases where pharmacotherapy is immediately indicated.13 Sleep disturbance is a feature of several physical illnesses. Educating patients about avoiding stimulants and creating an environment conducive to restful sleep can be effective, and this also provides an opportunity to promote positive lifestyle changes such as smoking cessation, regular exercise and a healthy diet.
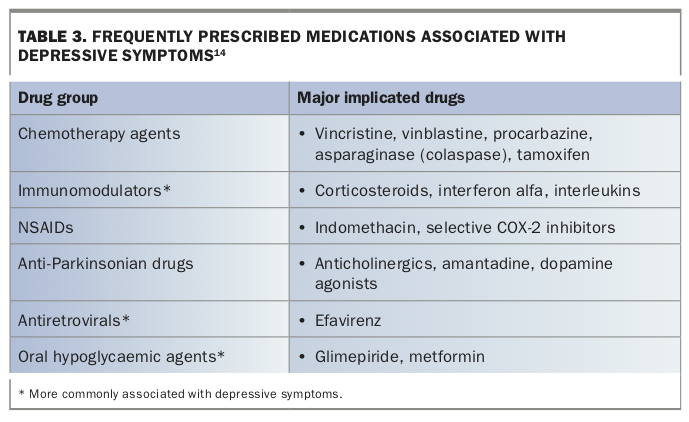
The GP should aim to withdraw any medications that might be contributing to depressive symptoms (Table 3).14 However, this may not always be possible, especially when there are no satisfactory alternative treatments.
{kind=link}
Any substance use problems must also be addressed. This includes alcohol, illicit drugs and other substances. Nicotine, caffeine, opiates and benzodiazepines can all disturb sleep-wake cycles and mood.
Psychological interventions
Cognitive behavioural therapy (CBT) and interpersonal therapy (IPT) are two focused, brief and effective psychological strategies for managing depression in patients with a medical illness. CBT aims to modify dysfunctional cognitions and behaviours related to depressive symptoms. Many GPs are familiar with CBT and may be competent in conducting this treatment, but IPT may be less well known. IPT can be useful for treating depression in people with a medical illness due to its focus on ‘role transitions’ and adjusting to changes in one’s circumstances. Clinical psychologists will be familiar with CBT and most will understand the principles of IPT.
Patients with difficulty adjusting to a sudden illness or an exacerbation of a chronic illness may also benefit from brief supportive psychotherapy or counselling, either with the GP or a psychologist. Some patients with chronic illnesses or with a history of trauma can develop maladaptive coping styles. These individuals may benefit from consideration of a longer-term treatment such as psychodynamic psychotherapy. A psychiatrist should be involved in decisions about such long-term treatment options for patients with medical illnesses.
Medications
There is no evidence supporting prescription of one antidepressant over another in the treatment of patients with depression and specific physical health problems.15 If pharmacotherapy is indicated, selective serotonin reuptake inhibitors (SSRIs) are generally preferred for their relative safety, efficacy and tolerability.12 Among SSRIs, citalopram has relatively few drug interactions. However, there are situations in which SSRIs should be used with caution. For example, SSRIs may increase the risk of gastrointestinal bleeding in patients taking NSAIDs. They may also cause or exacerbate hyponatraemia, especially in older people. In such cases, an antidepressant with a different mechanism of action may be preferred.
Older medications such as tricyclic antidepressants and monoamine oxidase inhibitors are effective but should be used with caution, particularly in people with cardiac conditions. A psychiatrist should be consulted before starting any of these medications in someone with a medical illness, because of their poorer tolerability, interactions with other medications and risks in the situation of an overdose.
Potential interactions between medications for depression and physical illnesses must be addressed. The most significant pharmacokinetic interactions to bear in mind when prescribing antidepressants are mediated through inhibition of the cytochrome P450 metabolising enzymes. These enzymes also metabolise many medications commonly prescribed for physical illnesses, including many beta-adrenergic blocking agents, NSAIDs, antihypertensive agents and proton-pump inhibitors. Pharmacodynamic interactions, such as the additive effect of SSRIs with serotonergic drugs, or mirtazapine with other sedating drugs, must also be considered when prescribing antidepressants to someone with a medical illness.
In patients receiving antidepressant treatment, the aim should be to titrate up to an effective dose. Once an effective dose has been reached, remission will generally require up to six weeks of regular treatment.
Specialist referral
GPs should strongly consider referring anyone with severe depression, suicidality or diagnostic uncertainty to a psychiatrist.13 Patients who do not respond to trials of two different antidepressants should also be referred to a psychiatrist. A specialist can advise on the helpfulness of physical treatments such as electroconvulsive therapy (ECT) or transcranial magnetic stimulation, which can bring about rapid improvement in patients with severe depression.13
Conclusion
GPs can efficiently and effectively assess patients with medical illness who present with depressive symptoms. Although it can be difficult to establish causation, considering the possible effects of a medical illness on a patient’s depression can help both with diagnosis and planning treatment. Support from psychologists and psychiatrists is generally advisable in complex cases. GPs have a broad range of clinical skills and the rapport they have with their patients can be most important. GPs remain ideally placed to assess and coordinate treatment for patients with a medical illness presenting with depressive symptoms. MT