UV radiation and ocular damage

The GP, as a front-line healthcare worker, will see patients who present with a variety of UV-related ocular conditions. General awareness and understanding will be helpful in providing appropriate counselling and referral, as required.
The human eye is routinely exposed to ultraviolet radiation (UVR), the main source being the sun. There is extensive evidence to support an association between a wide range of eye conditions and either a single acute episode or cumulative UVR exposure.1,2 UVR damage is likely to also reflect occupation and lifestyle choices and the level of care taken over time.2 Despite a range of past research initiatives, our understanding of the pathogenesis of sun-related ocular damage remains minimal at best.3
UVR is higher energy than visible light and therefore carries a more significant risk of damage. Importantly, UVR is outside of the human range of perception. The UV spectrum is categorised by wavelength as UV-A (400 to 320 nm), UV-B (320 to 280 nm) and UV-C (280 to 220 nm). As absorption increases with shorter wavelength, UV-B and UV-C are almost entirely absorbed by the ozone layer; however, most UV-A radiation (about 95%) passes through.4 Although mostly filtered out, UV-B remains biologically active and can penetrate the superficial layers of the skin and anterior tissue of the eye, leading to inflammation and photoageing. UV-B may also penetrate cell DNA, leading to mutation and skin cancer development. Although UV-A is lower energy radiation than UV-B and UV-C, the abundance of UV-A presents a significant concern, as it penetrates more deeply through skin layers. Consequently, UV-A radiation has been implicated in DNA oxidisation and immunosuppression.5
Although direct sunlight constitutes the main risk of exposure, other factors can lead to ocular damage. Scatter and reflection can contribute as much as 50% to the total ocular UVR exposure. As scattering is increased by clouds and haze (pollution), continued vigilance is required regardless of the weather. The degree of reflection depends on the surface and is relevant even when a person is facing away from the sun; the ground commonly reflects UV at less than 10%, and reflection from open water may reach 25%. Snow and ice are highly reflective for UV, at 94%; therefore it is essential that UV protection is considered in these conditions.6 Geography can have an impact on UVR exposure, with higher altitudes and lower latitudes being synonymous with increased UVR exposure and resultant UVR-related damage.6 Of particular interest, ocular exposure and UV-B burden are greatest in summer between 8 to 10 am and 2 to 4 pm. Both time periods fall outside the time traditionally considered highest risk for UV skin damage, again highlighting the need for constant vigilance.7
UVR-related ocular disease
UVR has been implicated as a contributing factor in a number of ocular conditions. Although patients will occasionally present to the GP with symptoms attributable to direct or excessive UV exposure, most conditions evolve gradually and without marked clinical features. An awareness of risk factors and typical clinical signs alongside general ocular observation represents the best opportunity for the GP to diagnose UVR-related damage in preparation for specialist treatment. This article aims to provide some context to potential UVR-related ocular disease for the GP in clinical practice.
UVR and the eyelids
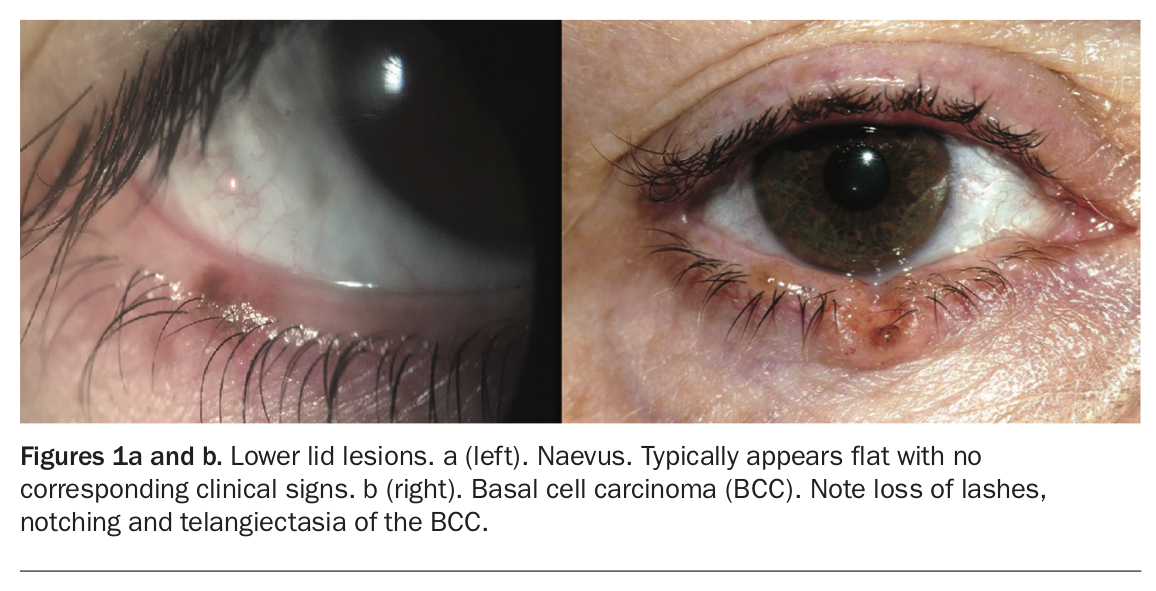
Basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) are relatively common malignant tumours of the eyelid (Figure 1).8 BCCs comprise about 90% of eyelid cancers and often present as a slowly forming reddish nodule (nodular BCC).9 Eyelashes may be absent from the area if the growth is along the lid margins. Due to protection provided by the eyebrow, BCCs most commonly appear on the lower eyelid and are medially located. Inflammation of the BCC with or without ulceration increases the risk of transformation into more aggressive tumour phenotypes. The appearance of SCCs on the eyelid ranges from a flat, reddish or flaky growth to a thickened, well-demarcated, raised reddish tumour surrounded by an inflamed area. Eyelid tumours rarely lead to metastases; however, some forms of BCC are locally aggressive (morpheaform, infiltrating and basosquamous subtypes) and early referral and treatment are essential. Factors associated with a poor prognosis include younger age, size, location at the inner canthi and recurrence.10 Both types of tumour can be removed surgically and rarely lead to further complications, although ongoing review is necessary.8
{kind=link}
There is strong evidence to suggest that the development of SCCs is attributable to extensive sun exposure over time. The relationship between UVR and risk of BCC is less well understood; however, evidence suggests that a person is more likely to be at risk of developing a BCC if they had significant UVR exposure before 25 years of age.9 These associations have been observed in several countries and point to the need for protection for young people, particularly those spending any significant time outdoors.9 Positively, the impact of strong sun-protection campaigns is now being recognised, and recent evidence suggests there has been a reduction in the incidence of sun-related skin cancer in these countries.
Ocular surface squamous neoplasia
Ocular surface squamous neoplasia (OSSN) encompasses a variety of diseases involving dysplastic squamous epithelial cells on the eye surface. Conjunctival intraepithelial neoplasia (CIN), a slow-growing tumour developing on the ocular surface, is the most common form. Its aetiology often involves a combination of environmental factors in a susceptible person. Notably, OSSN is significantly more prevalent in populations living within 30° of the equator, suggesting UVR is a major contributing factor.11
Patients are often unaware of the presence of OSSN unless the condition progresses to the moderate stage. An extended history of redness or localised inflammation represents a potential red flag for GPs, although direct diagnosis is often difficult due to wide variation on presentation. Lesions may be flat or elevated and may have associated feeder vessels. Corneal involvement as a result of advanced growth may result in a localised greyish, frosted appearance (Figure 2). Topical chemotherapeutic agents such as mitomycin, fluorouracil and interferon alfa-2b have gained popularity as primary treatments (off-label use), although surgical excision may be required. Regional lymph node metastasis has been noted in a small percentage of OSSN cases. Systemic metastases are exceedingly rare.12
{kind=link}
Pingueculae and pterygia
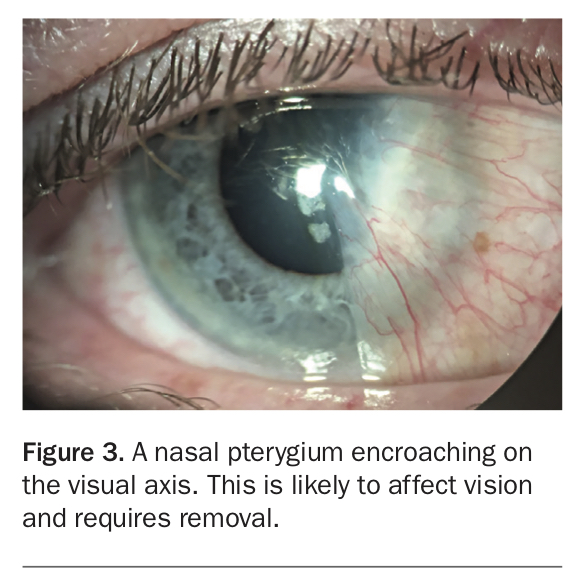
Pterygia appear as fleshy, vascular tissue that in time grows across the eye (Figure 3). Sun exposure, wind and dust may aggravate the condition leading to a consistent red, ‘angry’ appearance. Although the exact cause of pterygia is unknown, there is a significant link to outdoor work and both UV-A and UV-B exposure.13 Again, geography appears to also play a role in the development of the condition, which has a high prevalence between the 37° north and 37° south latitudes.13 This suggests that all people in Australia, particularly those who do not take adequate precautions against continued UV exposure, remain at increased risk of developing pterygia.
{kind=link}
Pterygia are commonly found on the nasal side of the eye and grow across the eye; they grow from the outside or lateral aspect in only a minority of cases. This is because light entering the eye tangentially is then focused across the anterior chamber of the eye, coming to a focus on the opposing nasal side where the concentration of UVR may be increased 20-fold as a result (the ‘Coroneo effect’).14 Depending on design, sunglasses may not effectively block these rays. Wrap-around sunglasses are ideal for minimising this risk.
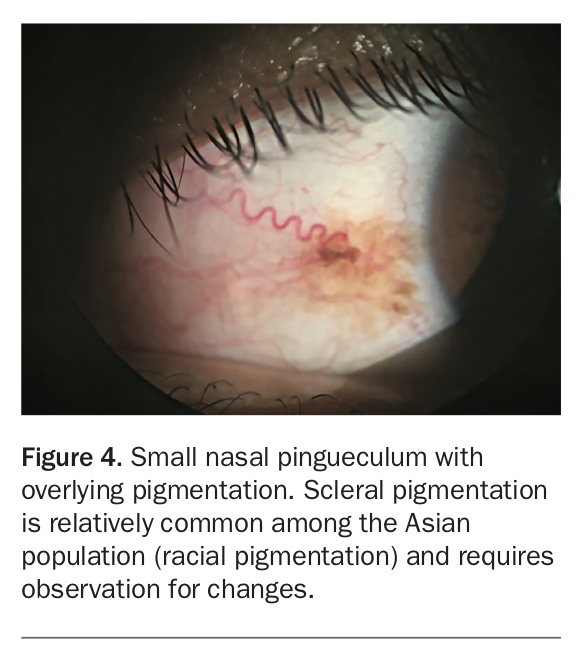
Pinguecula appear as raised, yellowish spots over the sclera. Although their presence may have an impact on blinking and lead to tear film abnormalities, the presence of pinguecula is largely a cosmetic concern. Once simply considered to be fatty deposits, pinguecula are a squamous metaplasia of the ocular surface epithelium. Evidence suggests a link to UVR as well as multiple other risk factors (Figure 4).1,2
{kind=link}
A pterygium may affect the tear film, leading to dry eye-like symptoms and variable vision. Further, pterygium growth may lead to corneal distortion and induce irregular astigmatism. In severe cases, vision is directly impacted by the pterygium covering the line of sight. The decision to surgically remove the pterygium depends on the size of the growth and degree of irritation and should be made in consultation with an ophthalmologist. The procedure of choice is dissecting the pterygium tissue before placing a conjunctival autograft over the nub of the pterygium. This procedure has dramatically reduced regrowth rates to about 1 to 2% and has significantly improved long-term cosmesis. Pingueculae are not usually removed due to their static nature.
An OSSN may occasionally present with a similar clinical appearance to a pterygium. If the diagnosis is unclear, specialist referral is indicated.
Ocular melanoma
Although ocular melanomas can present in any tissue of the eye, melanoma of the choroid is the most common primary intraocular malignancy in adults, accounting for about 5% of all melanomas. Unless growth has led to secondary changes, intraocular melanomas are often asymptomatic and identified sequentially during routine ophthalmic investigation. Retinal detachment leading to ‘flashes of light’ may occur because of increased traction of retinal layers. Tumours located below the fovea can lead to distortion of vision or loss of visual acuity. An understanding of risk factors is important for the GP. The Collaborative Ocular Melanoma Study found that ocular melanomas occurred more in Caucasians aged over 60 years.15 Patients with ocular pigmentation should be counselled to continue regular ocular examinations.
UV light exposure remains a contributing factor, although occupational exposure (e.g. welding) may further increase risk. Although less than 2% of patients show evidence of metastasis at diagnosis, over 40% of patients develop widespread disease, which is often fatal.15
Photokeratitis
Similarly to the way the skin can be damaged from an acute exposure to UVR, the eye itself can suffer from ‘sunburn’. This is photokeratitis and represents a superficial corneal burn. Colloquially, the condition is referred to as ‘snowblindness’ because it often occurs due to the UV-B reflection off snow. The condition routinely appears around six hours after acute exposure, and most cases will resolve relatively quickly over the following 24 to 48 hours. The patient will often experience general eye grittiness, increased tearing and sensitivity to light. Intense localised pain is rare but can occur. In severe cases, corneal swelling can lead to a temporary decrease in vision. If vision is unaffected, suitable treatment can be provided by the GP with artificial lubricants and rest. The patient should be counselled against further exposure during the healing process. Specialist referral is required if symptoms are prolonged.
Although predominantly resulting from significant exposure to natural light, photokeratitis can be caused by artificial light. Tanning beds and ‘welder’s flash’ are two examples of abnormal artificial UVR exposure that may cause the condition. It is possible that a single episode of photokeratitis may lead to long-term molecular and cellular changes, highlighting the need for counselling for at-risk individuals.16
The lens and retina
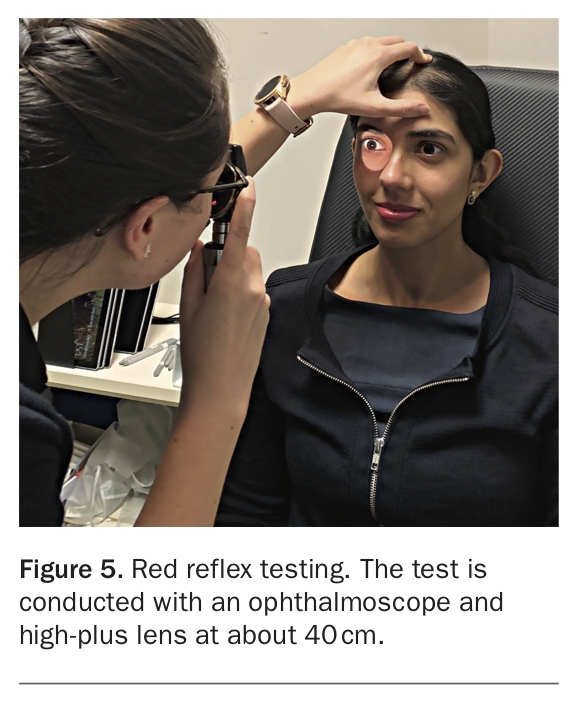
Cataracts are the main cause of reversible blindness throughout the world. As a cataract develops, the patient can be affected by increased glare, reduced contrast, colour vision changes and a decrease in best-corrected visual acuity. Progression is gradual except in cases associated with metabolic disorders such as diabetes. On examination, the pupil may appear cloudy. The use of an ophthalmoscope at about 40 cm will provide further clinical information. A cataract appears as a dull or diminished reflex (Figure 5).
{kind=link}
Several factors are linked to cataract formation including age, smoking and poor systemic health.17 Eighty percent of a person’s lifetime UVR exposure is reached before the age of 18 years, indicating this is a critical period for ocular protection.18 Although it is difficult to limit confounding factors within studies, evidence suggests that doubling the total UV-B exposure over time may increase the risk of cataract by as much as half again compared with people with low exposure.2 The WHO has suggested that the incidence of cataract may be reduced by at least 5% with the use of adequate UVR ocular protection.18
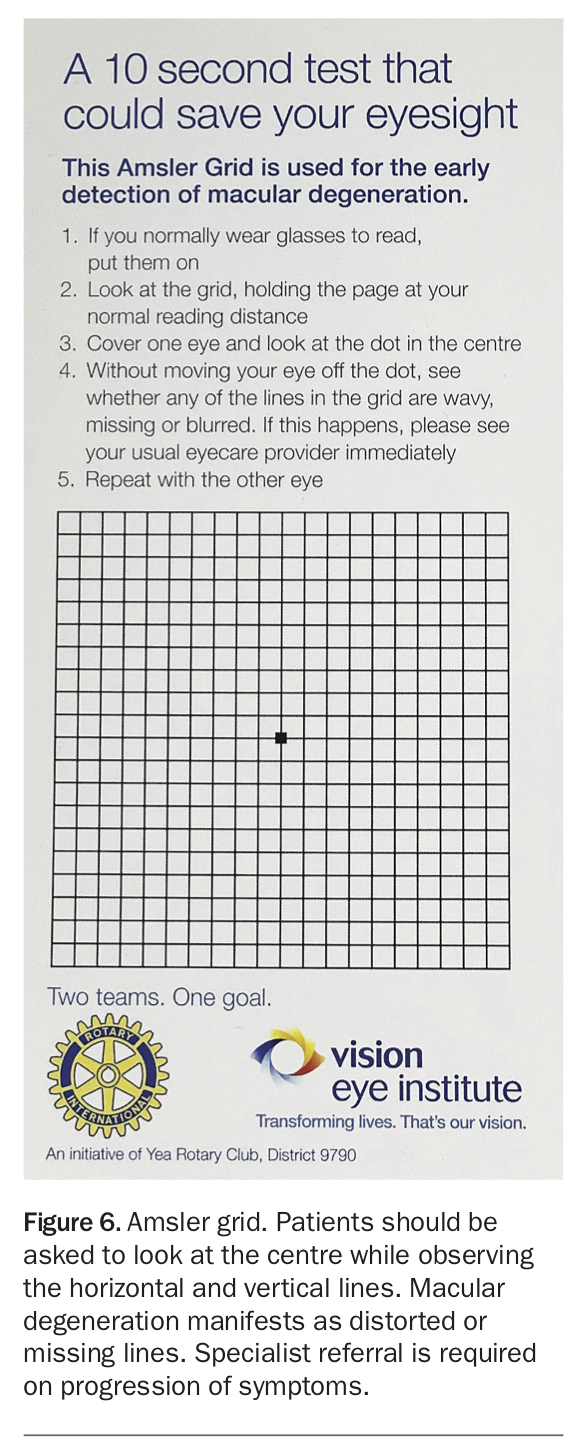
Macular degeneration (MD) is associated with UV exposure. A patient with MD may initially describe missing words repeatedly when reading or distorted central vision. Amsler grids, readily available from low vision speciality centres, may help diagnosis (Figure 6). High lifetime ambient UV exposure has been shown to be associated with increased risk of both cataract surgery and MD; however, even low UV exposure may be a contributing factor to MD.19 Additional epidemiological evidence also suggests a trend toward association between UVR and MD; however, further research is required to confirm this trend.20
{kind=link}
Much has been made recently of the potential damage from both industrial and toy lasers. Unprotected exposure to lasers often leads to permanent damage, resulting in reduced vision and/or paracentral visual scotomas. Immediate specialist referral is essential in suspected cases with a positive history of exposure; however, treatment options are limited.21 A recent systematic review of cases found that visual acuity remained worse than 6/12 in 55% of cases, representing a significant loss of vision.21
Protection
A recent study found that although more than half of the general population routinely wear sunglasses on a sunny summer day, only one-third of outdoor workers do so.22 Although about every seventh individual surveyed described never wearing sunglasses during leisure time, among outdoor workers it was one in three. Younger people were less likely to use eye protection, which is of greater concern with regard to long-term damage.
The primary form of protection promoted across all information campaigns is avoidance of UVR exposure. Although this is clearly the most effective form of protection, it is not practical, particularly in Australia where there are many opportunities for outdoor activities. There are a number of steps people can take to minimise UVR-related issues, however. Hats with a wide brim are helpful in reducing direct exposure. Effective UV-blocking lenses for patients requiring prescription glasses or equivalent sunglasses are essential at all times of the day. Depending on the characteristics of the frames and the distance the lenses sit from the eye, it is possible, however, that the glasses may only block as little as half the ambient UVR.23 A further practical risk is that the back surface of a sunglass lens itself may reflect an additional 25% of ambient UVR, further increasing the risk of ocular damage.24 Wrap-around glasses remove this concern, and more recent innovations include an additional back coating on lenses.
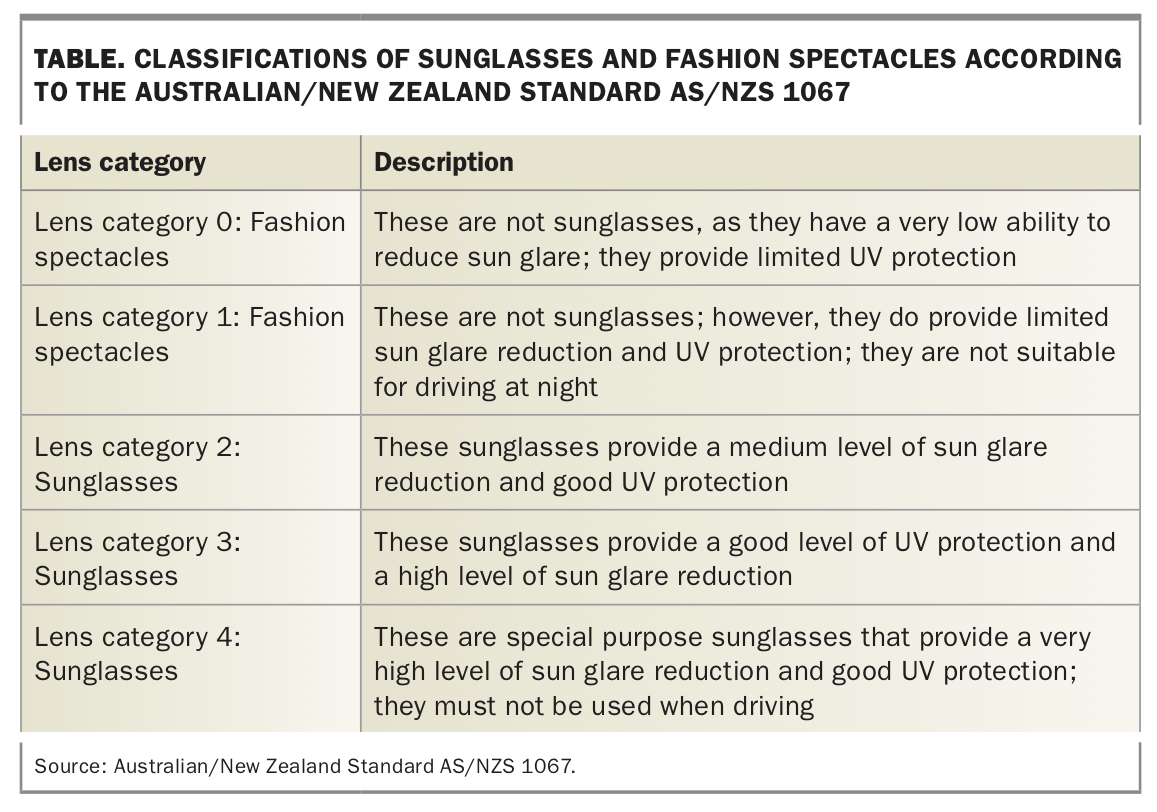
In July 2019, it became mandatory for all sunglasses sold in Australia to be tested and labelled according to the broader Australian and New Zealand standard (AS/NZS 1067.1.2016).25 The standard specifies several factors including lens dimensions, light transmission levels, optical quality and safety requirements. This allows the public to gain a better understanding of which lenses may be most appropriate. Currently, there are five categories ranging from 0 (fashion spectacles which provide limited to no UVR protection) through to category 4, which are special-purpose sunglasses designed for very high-level sun glare reduction and UVR protection (Table). Lens category 4 sunglasses are considered appropriate for mountain climbing or sailing, for example, but are not recommended for use while driving. Ideally, sunglasses should be at least category 2 and preferably category 3, which are designed for medium- to high-level glare reduction and good UVR protection.
{kind=link}
Tint and polarisation are two additional factors to be aware of. Tint represents a colour preference, although some tints are considered more relevant to certain activities. Brown tints, for example are considered a preferred choice for wearers who move between bright and low or shadowed environments, as may occur on a golf course. Importantly, the level of tinting does not represent the quality of UVR protection. Polarised lenses are specifically designed to provide additional benefits against glare, which may further aid visual and colour clarity. Polarised lenses are not essential, although they may be of benefit if the wearer spends significant time participating in high-glare activities (e.g. on water). Polarised lenses reduce glare, but this is not equivalent to protection from UVR. Anyone purchasing sunglasses should consult their optician to ensure they choose the most appropriate protective lenses.
Conclusion
Regular review is essential in patients with suspected UVR-related ocular damage. Additionally, photographs of eyelid or surface conditions are helpful to track the course of the condition. Surgery may be indicated in marked cases; however, this should be undertaken only after the potential risks and benefits of a procedure are discussed with the patient.
With a relatively high standard of living in Australia, people are living longer lives, which raises the risk of both acute and cumulative exposure of the eyes to UVR, and may in some circumstances lead to potentially vision-altering conditions. Being aware of this risk and using direct measures such as sunglasses and headwear at appropriate times offers the best protection and helps ensure eye health. The GP, as a front-line healthcare worker, sees patients who present with a variety of UVR-related ocular conditions, and general awareness and understanding are helpful in providing appropriate counselling and referral, as required. MT