An update on travel vaccinations

Immunisation
Many travellers visiting low-income countries or travelling in groups or on cruise ships will experience a travel-related ailment, so a personalised pretravel health consultation is essential to assess the risks for an individual traveller and to offer appropriate advice and vaccinations. In some instances, vaccinations will be required for crossing international borders.
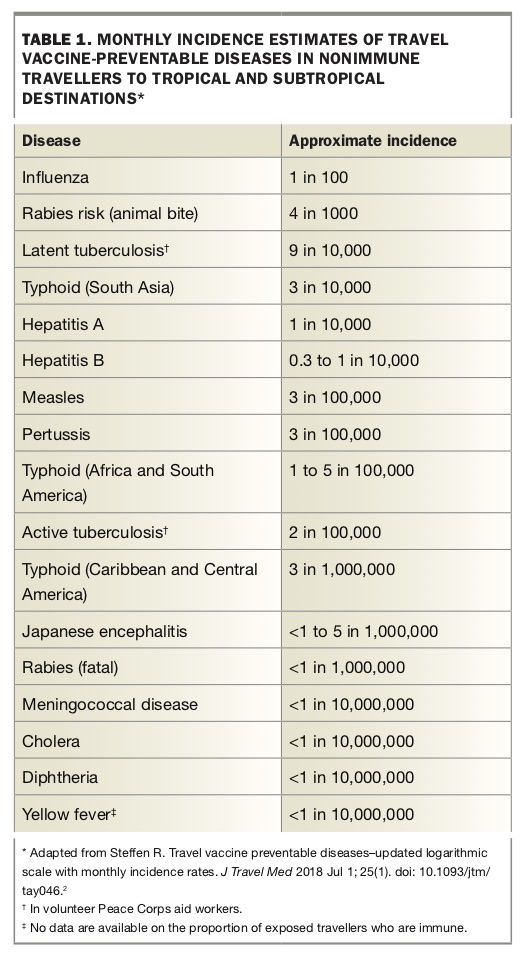
As travellers are able to cross borders and visit all points of the globe, they can be exposed to various hazards. It has been estimated that up to half of all travellers visiting low-income countries for one month will experience some travel-related ailment.1 Recently updated estimated monthly incidence rates of vaccine-preventable diseases in nonimmune travellers show that influenza is now the most common of these diseases, affecting 1% of travellers per month (Table 1).2 This highlights the importance of discussing the potential benefits of influenza vaccination with patients who are intending to travel, especially those travelling in groups or on cruise ships.
{kind=link}
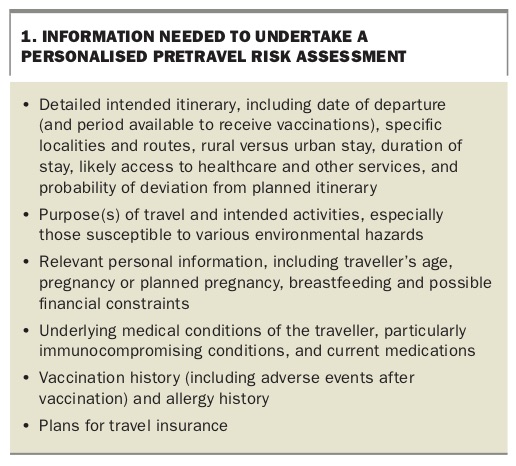
Illness among travellers depends on a variety of factors that the health practitioner needs to ascertain during the pretravel consultation. To provide appropriate travel health advice, practitioners must obtain sufficient information from the traveller to enable an adequate personalised risk assessment. A complete risk assessment should cover the individual, the means of travel, the destination and, ultimately, any intervention that will be used (Box 1).
{kind=link}
Once the risk assessment has been completed, the pretravel health consultation generally consists of three main areas: vaccination, education and prescribing chemoprophylaxis and travellers’ medical kits.
Travel vaccinations can be divided into three groups:
- routine childhood or adult vaccinations
- required vaccinations – for crossing international borders
- recommended vaccinations – according to risk of disease.
This article provides an update on the vaccinations that are currently licensed in Australia and relevant to the pretravel consultation.
Routine childhood or adult vaccinations
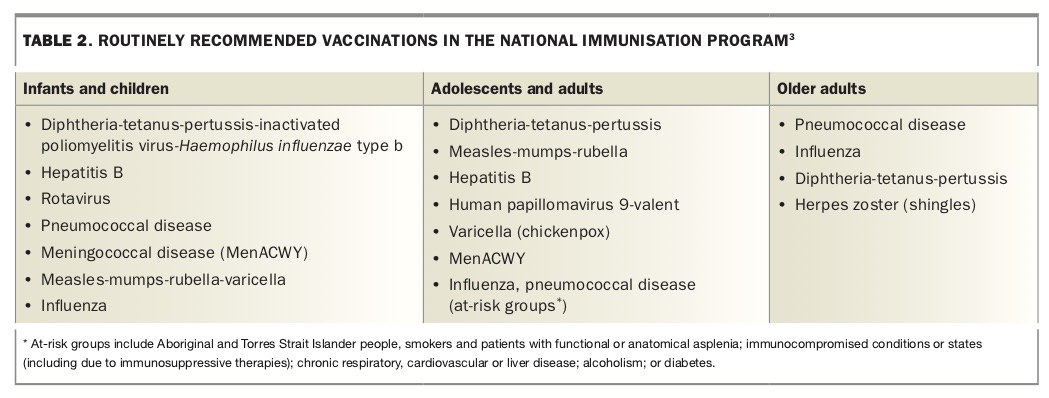
It is important to check that all travellers are up to date with their routine age-related vaccinations, according to the National Immunisation Program (Table 2). If not, these should be updated, as the risk of exposure to routine vaccine-preventable diseases is higher than the risk of exposure to more exotic tropical infections, such as Japanese encephalitis or typhoid, during international travel. Relevant routine vaccinations include those for hepatitis B and measles-mumps-rubella (MMR) in young adults, and influenza in young children, ‘at risk groups’ (e.g. those with chronic respiratory disease or immunosuppression) and the elderly. All infants and children aged less than 2 years are also strongly recommended to receive vaccination against meningococcal B disease.3
{kind=link}
Most Australian children born since 2000 have been vaccinated against hepatitis B under the National Immunisation Program. Hepatitis B vaccination is recommended for people undertaking long-term (more than four weeks) or frequent travel to regions of high or intermediate hepatitis B endemicity, including Central and South America, Africa, Asia and certain destinations in Oceania.3 As well as the region of travel, the behaviour of travellers while abroad is important in determining their individual risk of hepatitis B exposure, as they may be exposed to the virus through bloodborne (including during emergency medical or dental procedures) or sexual routes.4
There are ongoing outbreaks of measles and mumps in Europe and the Americas, with most outbreaks in Australia being traced back to infected returning travellers who were inadequately vaccinated.3 Overseas travellers are now recommended to have either documented evidence of two doses of measles-containing vaccine given at least four weeks apart or serological evidence of immunity to MMR.3
Required vaccinations
Yellow fever
The vaccine used for the prevention of yellow fever, which is a mosquito-borne illness, can only be administered by registered yellow fever vaccination providers. The practitioner needs to determine if the traveller will be at risk of yellow fever at the destination and/or if vaccination is required under the International Health Regulations (IHR).5
Some countries have specific yellow fever vaccination requirements or changing requirements that are not explained by looking at the yellow fever maps.6 It is therefore important to understand the full details of the traveller’s itinerary, including countries that may be briefly transited through, to have up-to-date data on yellow fever transmission and to be aware of current vaccine recommendations.
As there are rare but significant adverse events associated with yellow fever vaccination (including an anaphylaxis rate of 1.3 per 100,000 doses administered and a rate of vaccine-related neurotropic or viscerotropic events of one to two per 1,000,000 doses administered), the risk of these events must be balanced against the true risk of exposure to yellow fever. If, on balance, the risk of significant vaccine-related adverse events is high (e.g. the traveller is aged over 60 years and is undertaking low-risk travel), an exemption or waiver certificate from the IHR requirements may need to be considered.7
The WHO has updated its advice regarding the duration of immunity from yellow fever vaccination, which was previously 10 years. As per Annex 7 of the IHR, a single dose of a yellow fever vaccine approved by the WHO is sufficient to confer sustained immunity and lifelong protection against yellow fever disease in most healthy adults and children.8 Although 10-yearly boosters are no longer required for international travellers, it is probably prudent to check individual country requirements, as not all countries are yet conforming to the updated WHO advice. Furthermore, some data suggest that vaccination of pregnant women and people with lowered immunity, such as those with HIV infection, may not provide lasting protection, and these people therefore require a booster vaccination.8
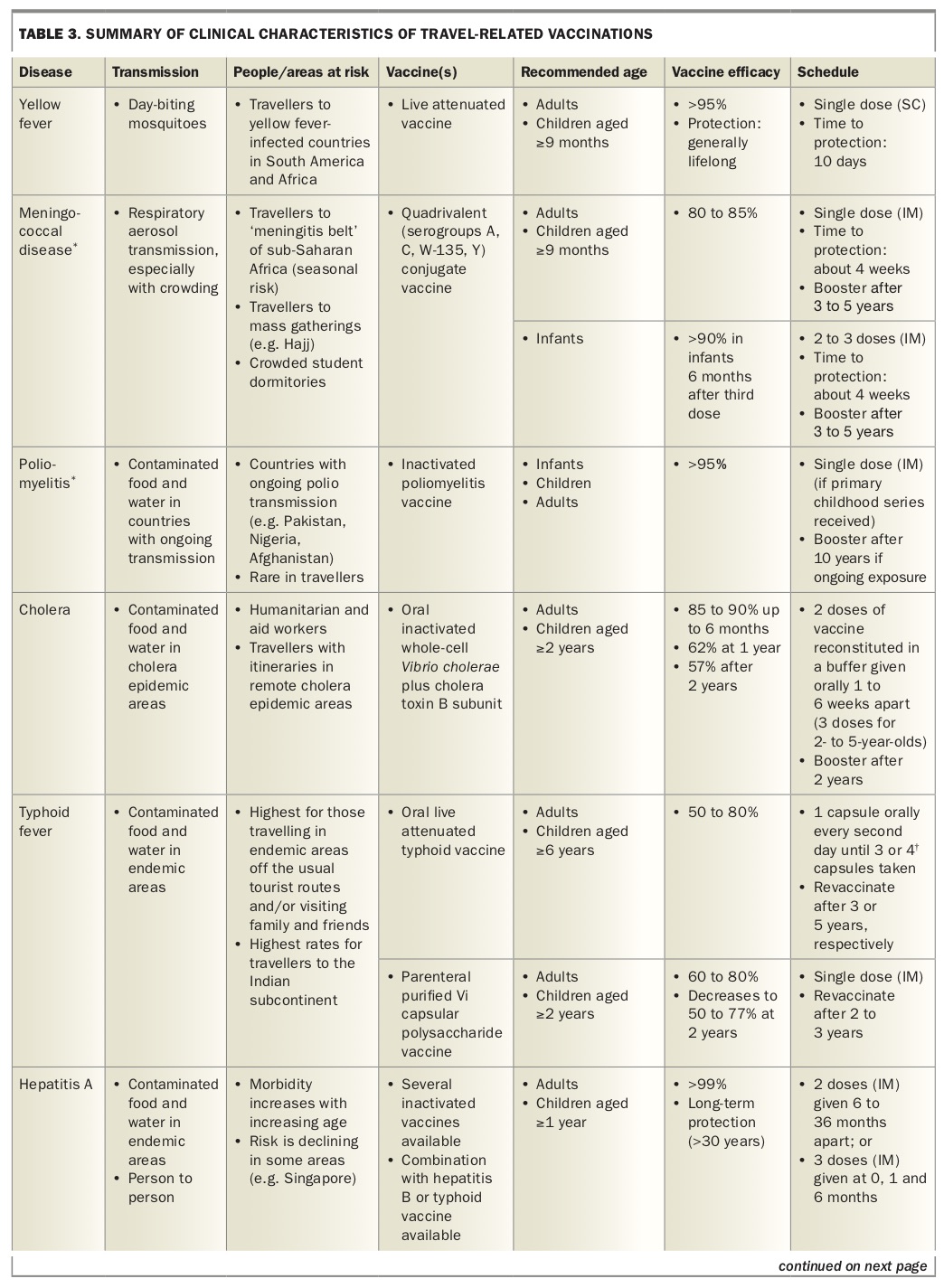
Table 3 and Table 3 Pt 2 summarises the yellow fever vaccine attributes and scheduling. The International Certificate of Vaccination or Prophylaxis (ICVP) should be completed for the traveller. This certificate becomes valid 10 days after the day of vaccination and remains valid for life.
{kind=link}
{kind=link}
Meningococcal disease
The quadrivalent meningococcal (MenACWY) vaccine is included in the ‘required’ vaccination category because it is required by Saudi Arabian authorities for religious pilgrims, including those travelling for the Hajj. Meningococcal meningitis is caused by the bacteria Neisseria meningitidis, which is transmitted from human to human via respiratory droplets, especially in crowded conditions. It is endemic in sub-Saharan Africa (the ‘meningitis belt’), which has the highest rates of the disease worldwide. During epidemics in this region, the incidence can approach 1000 per 100,000 people, or 1% of the population.7
The conjugate MenACWY vaccine should be used in preference to the polysaccharide MenACWY vaccine, as the conjugate vaccine provides a longer duration of immunity and also generates cell-mediated immunity, reducing nasal carriage of the bacteria. Two of the three available conjugate MenACWY vaccines are recommended for use in infants from 6 weeks of age, and the other from 9 months of age (Table 3 and Table 3 Pt 2 and Table 4).3
{kind=link}
Poliomyelitis
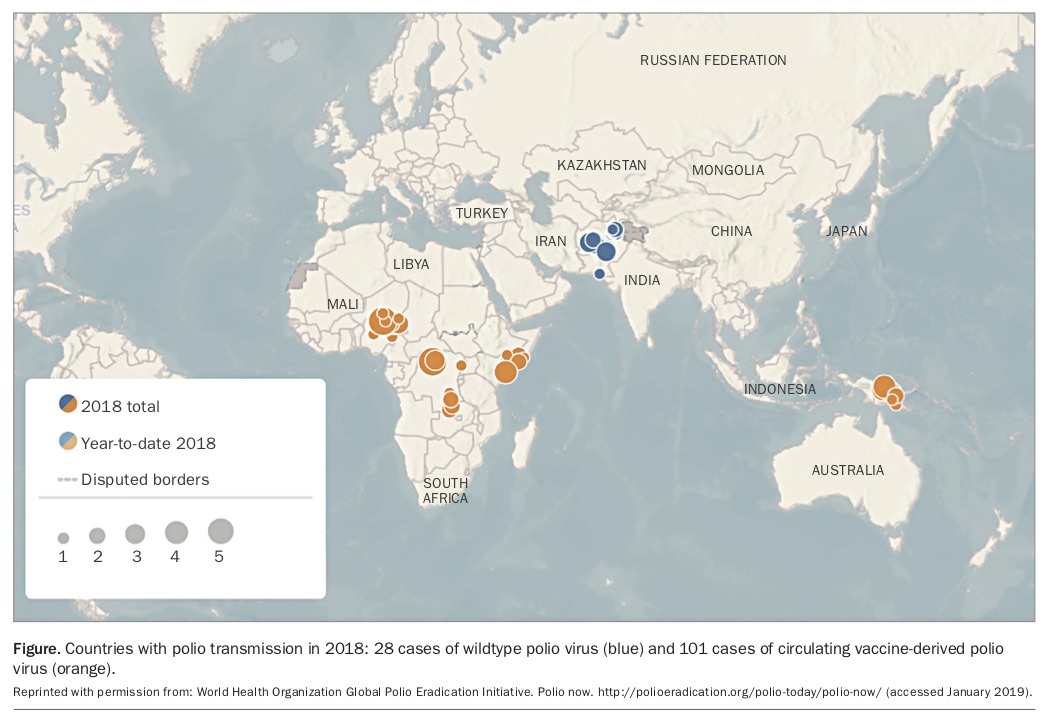
Poliomyelitis is rare in travellers. Pakistan, Nigeria and Afghanistan are the only three countries to have had active wildtype polio virus transmission between 2016 and 2018 inclusive.9,10 Niger, Nigeria, Somalia, Democratic Republic of the Congo and, more recently, Papua New Guinea have seen a return of polio because of circulation of vaccine-derived virus (Figure 1).9,10
{kind=link}
Under the IHR, all long-term visitors (those staying more than four weeks) from Afghanistan, Nigeria, Democratic Republic of the Congo, Kenya, Niger, Pakistan, Papua New Guinea and Somalia must have documented proof of vaccination with an inactivated poliomyelitis vaccine within the four weeks to 12 months before departing from these polio-infected countries.10 Practitioners need to ensure that such travellers are provided with an ICVP in the form specified in Annex 6 of the IHR to record their polio vaccination and serve as proof of vaccination.10
Recommended vaccinations
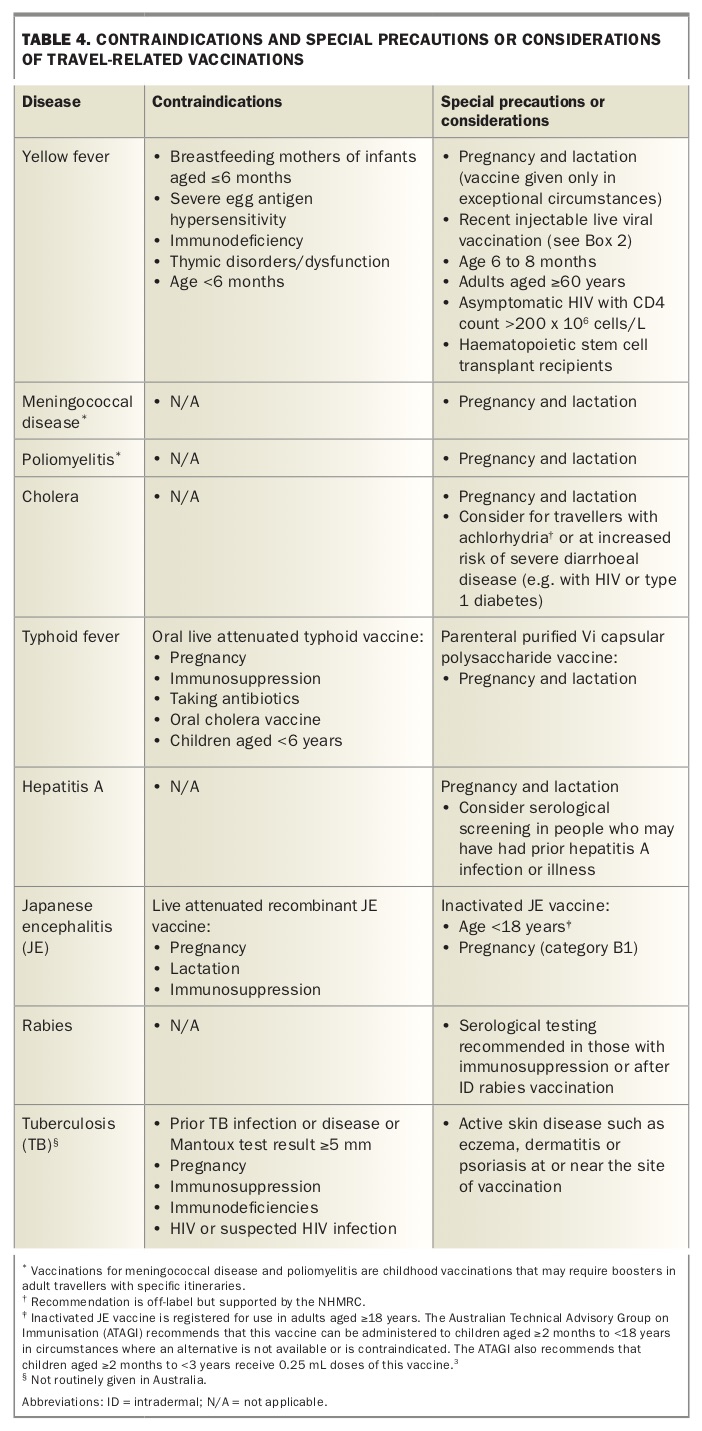
Recommended vaccinations include those for vaccine-preventable diseases transmitted through contaminated food and water or from person to person via faecal–oral routes (cholera, typhoid fever, hepatitis A and poliomyelitis), mosquito bites (Japanese encephalitis and yellow fever), infected animal bites (rabies) and respiratory droplets (influenza, meningococcal disease and TB). Table 3 and Table 3 Pt 2 and Table 4 summarise the attributes, scheduling and contraindications for recommended vaccinations, which are prescribed according to the risk assessment undertaken for the traveller. As noted above, some recommended vaccinations are also required for crossing international borders.
Cholera
Cholera is rare in travellers, as most do not visit areas with active cholera transmission. Up to an estimated two cases occur in a million western travellers.3,11 Vaccination should be considered for humanitarian and aid workers and those with itineraries in remote cholera epidemic areas.
The inactivated oral cholera vaccine is also recommended for travellers who have a higher risk of severe or complicated diarrhoeal disease and those at high risk of acquiring diarrhoeal disease, including people with poorly controlled or complicated diabetes, inflammatory bowel disease, HIV infection or other immunocompromising conditions, significant cardiovascular disease or primary or secondary achlorhydria.3 In this group of travellers, cholera vaccination can be used off-label for reducing the incidence of diarrhoea caused by Escherichia coli, for which the vaccine gives some cross-protection.11 The overall reduction in risk is modest but possibly significant in these individuals.
Typhoid
The risk of exposure to Salmonella enterica serotype Typhi is highest for people travelling off the usual tourist routes and those visiting family and friends.7 Highest rates of the disease are found in those travelling to the Indian subcontinent.7
There are two typhoid vaccines licensed in Australia: an oral live attenuated vaccine and a parenteral (injectable) Vi polysaccharide antigen vaccine. These vaccines have similar protective efficacy (50 to 80%) against S. typhi, although the injectable vaccine provides no cross-protection against S. paratyphi B, whereas the oral vaccine does.12 S. paratyphi B is more common in South and Central America.
The oral typhoid vaccine strain may be destroyed by gastric acid, so the capsules must be swallowed whole rather than chewed or opened. There should be an interval of at least eight hours between administration of the oral typhoid vaccine and the inactivated oral cholera vaccine, as the buffer in the cholera vaccine may affect transit of the typhoid vaccine capsules through the gastrointestinal tract.
The oral typhoid vaccine may also be susceptible to inactivation by some antibiotics and antimalarial agents (including doxycycline). If the oral vaccine is used, it is recommended that vaccination be timed so that the last dose of vaccine is administered at least three days before starting antibiotics. Unlike injectable live vaccines, the oral live typhoid vaccine does not interact with other injectable live vaccines, but its use is contra-indicated in immunocompromised and pregnant people (Table 4).
Hepatitis A
The risk of acquiring hepatitis A infection has continuously reduced over the past four decades and is now about one per 10,000 travellers per month, depending on destination and style of travel in hepatitis A endemic countries.2 Morbidity from this infection increases with age, with a case-fatality rate of 1.8% in people older than 50 years.7
Several inactivated hepatitis A vaccines are licensed in Australia, all of which are highly efficacious, well tolerated and provide long-term protection (at least 30 years) in both children and adults, providing a complete course is given.2,8 Hepatitis A vaccine is also available in combination with hepatitis B or typhoid vaccines. Serological screening should be considered in people who may have had prior hepatitis A infection or illness.
Japanese encephalitis
This rare viral disease, which infects the brain with potentially devastating complications, is transmitted by night-biting mosquitoes in Asia and parts of the western Pacific. It is generally viewed as an infection of agricultural areas (risk correlates with exposure in endemic areas, which are usually rural). Most cases (more than 99%) of Japanese encephalitis are mild or asymptomatic. The case-fatality rate is 20 to 30% in symptomatic individuals (up to 50,000 deaths are reported annually), with another 30 to 50% having severe neurological, cognitive or psychiatric sequelae.7,13 At least 75% of cases occur in children aged 14 years or younger, with an overall incidence of five to 50 cases per 100,000 children per year in Asian populations.7,13
The Japanese encephalitis vaccination recommendations for people travelling to Asia and Papua New Guinea are customised according to the season of travel, regions to be visited (urban or rural), duration of travel and extent of outdoor activities.3 There are two licensed Japanese encephalitis vaccines in Australia: a two-dose vero-cell-derived inactivated vaccine, given at days 0 and 28; and a single-dose live attenuated recombinant vaccine. The two-dose inactivated vaccine schedule should be completed at least one week before exposure, whereas the recombinant vaccine should be administered in adults at least two weeks before exposure. There is an age-dependent need for boosters of each vaccine (Table 3 and Table 3 Pt 2 and Table 4).
A rapid two-dose schedule (seven days apart) for the inactivated vaccine has been recently approved in Europe for adults aged 18 to 65 years if time does not allow for a four-week interval between doses, but this is not yet approved in Australia.13
Rabies
Rabies occurs in more than 150 countries and territories globally. It is almost universally fatal in humans, with 59,000 deaths occurring worldwide each year, mostly in Asia and Africa.14 The rabies virus is transmitted through bites from infected animals; mostly dogs, but also bats, cats and monkeys. The rate of rabies exposure for travellers is at best an - estimate and may range from 16 to 200/100,000 travellers.7 Of people who are bitten by suspected rabid animals, 40% are children aged under 15 years.15 Every year, more than 15 million people worldwide receive postexposure vaccination to prevent the disease.15
Pre-exposure prophylactic (PrEP) vaccination provides partial immunity against the rabies virus. The standard course is three doses given on days 0, seven and 21 or 28, either intramuscularly or intradermally (off-label use). In the event of an exposure, two additional doses of vaccine, given three days apart, are still required. The WHO has recently issued revised recommendations that make PrEP available in just two doses, given on days 0 and seven; this course is only to be used when there are time constraints and with the proviso that a third dose is given within a year.2,14 This two-dose schedule has not yet been approved in Australia by the TGA or endorsed by the NHMRC; neither has intradermal administration of the rabies vaccine, despite this route being endorsed by the WHO.14 If the intradermal route is being considered, the NHMRC does provide guidance on the factors that need to be taken into account.3
Routine serological testing for rabies after intramuscular PrEP vaccination is not usually necessary. However, people who are immunocompromised or who received intradermal PrEP vaccination should have their rabies virus neutralising antibody titres determined 14 to 21 days after the third dose of vaccine, and a further dose should be given if the titre is reported as inadequate (i.e. less than 0.5 IU/mL). Serological testing should then be repeated and, if titres remain below 0.5 IU/mL, expert advice should be sought.3
Tuberculosis
Young children travelling to countries with a high incidence (more than 40 cases per 100,000 population per year) of tuberculosis (TB) for an extended period are at increased risk of acquiring TB and developing severe disease.3,16 The only existing vaccine against TB, the bacille Calmette-Guérin (BCG) live vaccine, which was created in 1921, has variable protective efficacy.17
As BCG vaccination does not prevent primary infection per se, nor reactivation among those already infected with TB (e.g. latent TB), the role of BCG vaccination in preventing overall transmission is limited.17 However, there is strong evidence that BCG vaccination in childhood (before 5 years of age) provides at least 90% protection against severe disseminated forms of TB disease, including miliary and meningeal TB, in young children, but that this protection declines with increasing age.18 As TB can be difficult to diagnose in young children, and progression to disseminated disease can be rapid, they are therefore the primary target for the use of BCG vaccine.
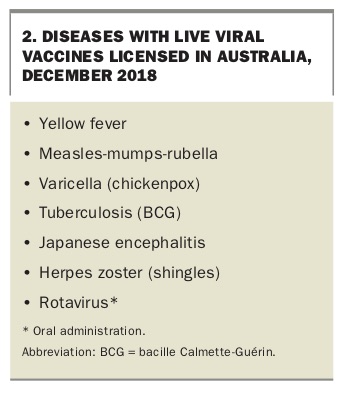
For child travellers who require the BCG vaccine, the following precautions should be considered when scheduling their vaccination visits. First, BCG vaccine should preferably be given at least three months before entry into endemic areas; however, as this is rarely practical for people returning to visit their families, it should still be offered at any time before departure. Other injectable live viral vaccines (Box 2) should be administered either concurrently or with a minimum four-week interval before or after BCG vaccination.3 Second, tuberculin skin testing (Mantoux test), performed by a trained and accredited healthcare practitioner, is recommended before administering the BCG vaccine for all individuals except infants aged less than 6 months.3 The response to tuberculin testing may be depressed for as long as four weeks after measles infection or administration of MMR vaccine,3,19 and those interpreting the results of the tuberculin test should be aware of any other recently administered live injectable vaccines.19
{kind=link}
Conclusion
It is essential to have a sound knowledge of the geographical, climate, cultural and other conditions that pose a risk to individual travellers, to alert them to these risks and to inform them how to avoid or minimise harm. This must be done in a fashion that does not frighten or discourage the traveller. A thorough pretravel preparation and medical consultation can mitigate avoidable health and safety risks.
An initial risk assessment needs to be undertaken to tailor the discussion to the relevant risks identified for the traveller. Recommendations for vaccinations are easy to find, but determining the actual degree of risk is the advice that practitioners are providing. This must take the form of a conversation with the traveller, as all travellers will have varying levels of risk acceptance. The correct interventions can then be chosen based on the discussion and risks.
Practitioners should be aware that vaccination costs can add up to as much as the traveller’s plane fare. Discretion is the byword; the risk and consequences of a severe anaphylactic or adverse reaction to vaccination must be considered, but it must also be recognised that giving a vaccination may save the person’s life. MT
COMPETING INTERESTS: None.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.