Insomnia treatment. Improved access to effective nondrug options

Dr Sweetman is a Research Associate at the Adelaide Institute for Sleep Health and the National Centre for Sleep Health Services Research, Flinders University, Adelaide.
Dr Lovato is a Senior Research Fellow at the Adelaide Institute for Sleep Health and the National Centre for Sleep Health Services Research, Flinders University, Adelaide.
Ms Haycock is a PhD Candidate at the Adelaide Institute for Sleep Health and the National Centre for Sleep Health Services Research, Flinders University, Adelaide.
Professor Lack is an Emeritus Professor in the College of Education, Psychology and Social Work and the National Centre for Sleep Health Services Research, Flinders University, Adelaide, SA.
Sleep disorders
Mental health
Insomnia is a common disorder managed in Australian general practice. The RACGP recommends cognitive and behavioural therapy for insomnia (CBTi) strategies as the first-line treatment. There are multiple simple and effective CBTi options accessible to Australian general practitioners and patients, but these are often underused.
- Insomnia is a common, debilitating and costly disorder managed in Australian general practice.
- Sedative-hypnotic medications are associated with potential side effects, adverse events and long-term dependence and are a suboptimal management strategy.
- The RACGP recommends cognitive and behavioural therapy for insomnia (CBTi) strategies as first-line treatment.
- Australian general practitioners can access multiple CBTi strategies, including effective self-administered, online, nurse- or GP-administered CBTi, or pathways for referral to a psychologist trained in treating insomnia.
- An NHMRC research program is underway to explore whether the management of insomnia in general practice can be improved in line with RACGP guidelines. GPs interested in participating in this research are encouraged to contact the authors ([email protected]).
Chronic insomnia is characterised by difficulties initiating or maintaining sleep, with associated daytime impairments, lasting for at least three months.1 Insomnia is the most common sleep disorder and impairs the lives of 10 to 30% of the Australian population, which, at a conservative estimate, equates to 2.5 million people. It costs Australia $11 billion annually due to its negative impacts on physical and mental health, healthcare costs and reduced productivity.2 Insomnia is a risk factor for depression and anxiety and contributes to 2.5- and twofold increases in motor vehicle and workplace accidents, respectively.3,4
Chronic insomnia is well recognised to be perpetuated by underlying psychological or behavioural causes. These require strategic behavioural and cognitive modifications to break the cycle of poor sleep habits and self-fulfilling worry about chronic poor sleep. However, 90% of patients presenting to general practice with insomnia are prescribed sedative-hypnotic medications, with a quarter of a million Australians consuming these medications each night, despite widespread recognition that this is suboptimal clinical practice.5,6 Patients seeking treatment often expect to receive sedative-hypnotic medications (e.g. temazepam, diazepam, zolpidem, zopiclone), which are quick to prescribe but are associated with high rates of adverse cognitive and psychomotor side effects. These include adverse physiological effects; a heightened risk of hepatic, renal, respiratory and cardiac disorders; daytime sedation; cognitive impairments; an increased risk of falls among the elderly; and the development of dependence and withdrawal effects after long-term use.7,8
Assessment of insomnia symptoms
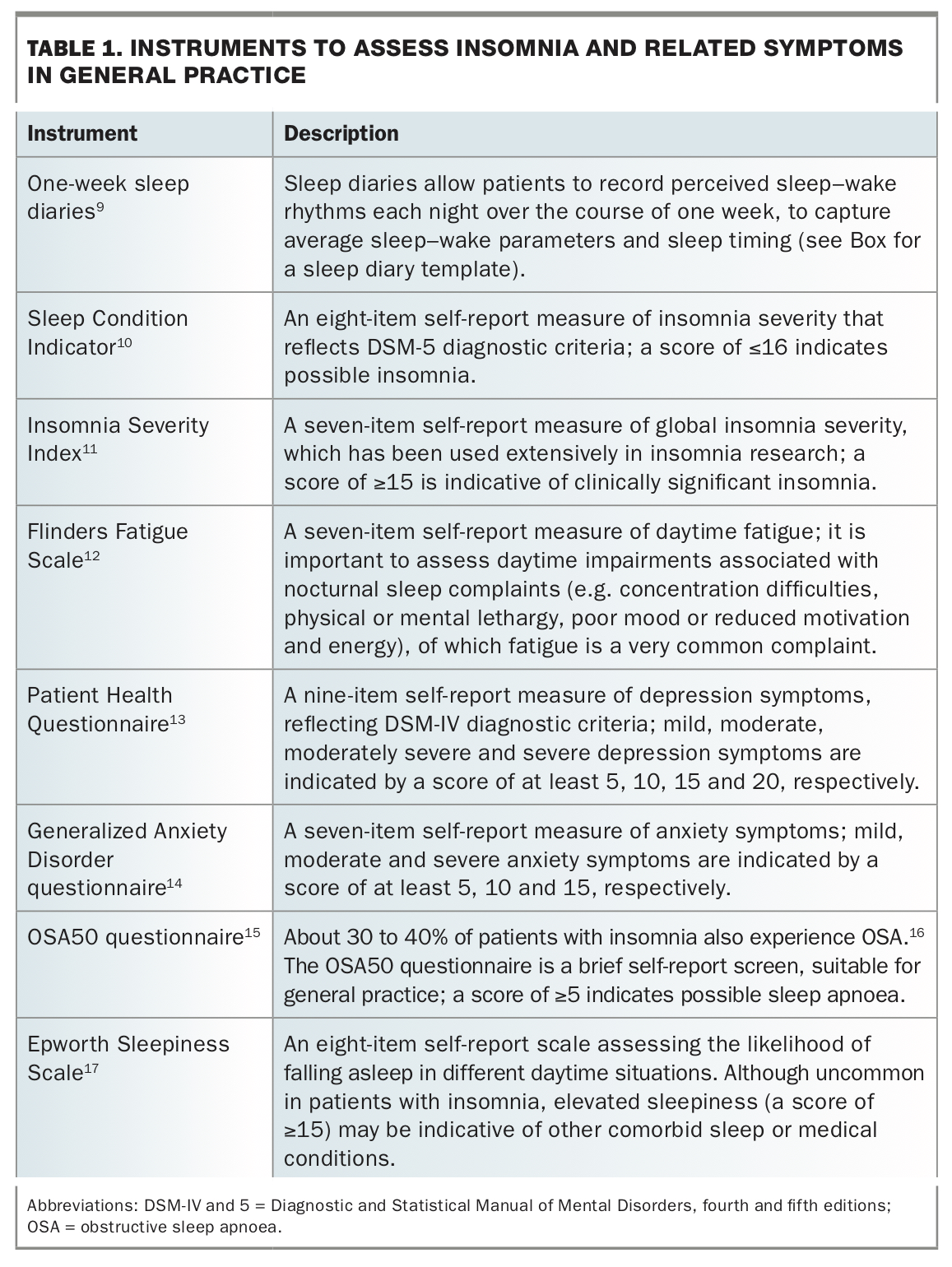
Insomnia is diagnosed according to self-reported difficulties in falling asleep or maintaining sleep, or early morning awakenings, and associated daytime impairments.1 Insomnia can be classified as acute (less than three months) or chronic (three months or longer). There are several simple self-report tools that can be used to screen for insomnia and related disorders or symptoms in general practice (Table 1).9-17 When assessing a patient for insomnia, it is also important to consider the contribution of other co-occurring medical or psychiatric symptoms, medications, alcohol and recreational drug use and other lifestyle factors.
{kind=link}
Recommended management of insomnia
The RACGP guidelines recommend that cognitive and behavioural therapy for insomnia (CBTi) strategies should be employed as the first-line treatment for both acute and chronic insomnia.8 CBTi includes a suite of therapeutic strategies employed and modified over four to 12 consecutive weekly sessions to gradually target the maladaptive psychological, behavioural and physiological processes that underpin the patient’s insomnia.7,18,19
Because CBTi targets the specific underlying causal factors of insomnia, this treatment is associated with minimal side effects, and improvements are sustained far beyond therapy cessation.20-22 The most common side effect of CBTi is a small increase in feelings of daytime sleepiness during the initial one to two weeks of bedtime restriction therapy.20 However, these feelings of sleepiness quickly dissipate as sleep is gradually consolidated and time in bed is extended after the first two weeks of restriction. CBTi is also effective in patients with comorbid medical or psychiatric symptoms, in older adults and when administered in general practice settings.22-25
Treatment options for insomnia
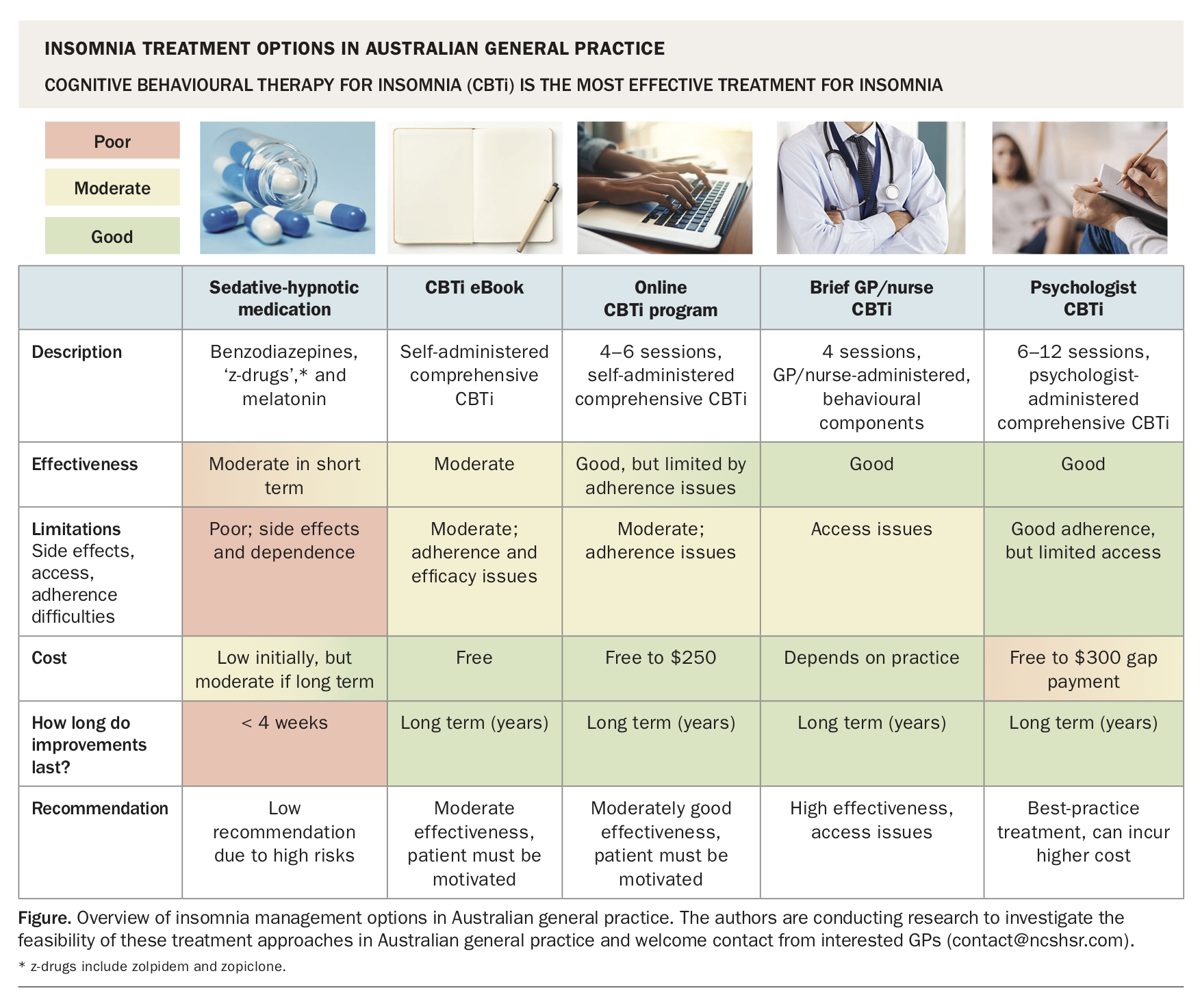
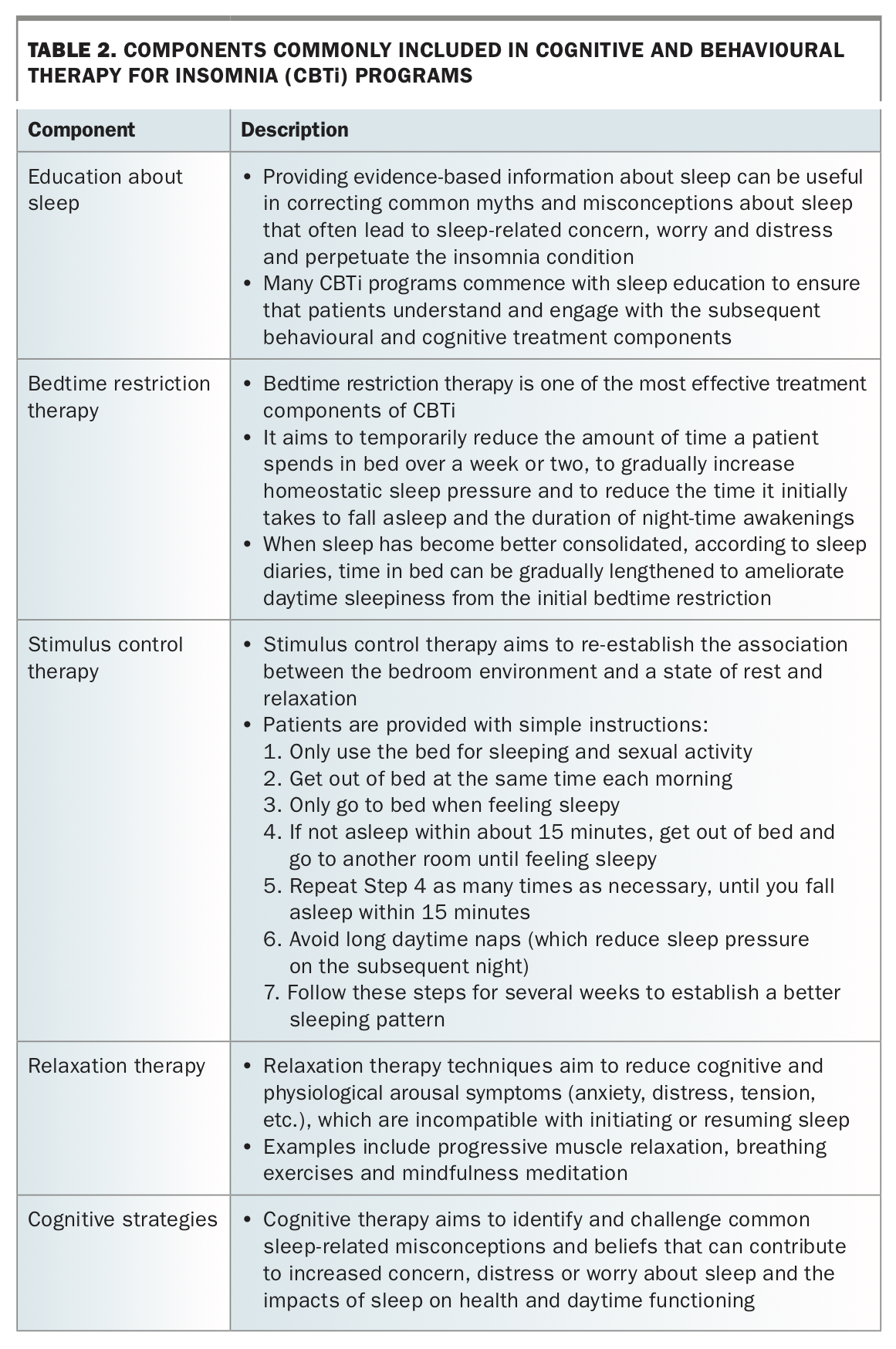
GPs, who are at the forefront of health service delivery, are ideally placed to manage insomnia. There are several evidence-based treatment approaches, including education about sleep, digital CBTi, CBTi administered in general practice and referral to a psychologist who specialises in CBTi (Figure).26 Each treatment approach is described below. It is recommended that the GP and patient work in a collaborative manner to select the treatment option best suited to the individual patient, based on his or her clinical profile and personal preferences. Table 2 provides an overview of treatment components commonly included in CBTi programs.
{kind=link}
{kind=link}
Education about sleep
There are many myths and misconceptions about sleep that make patients vulnerable to the development and perpetuation of insomnia, such as preconceptions about the amount of sleep one should obtain and the notion that awakenings during the night are pathological.27 Anecdotally, many individuals with symptoms of insomnia report education about sleep to be therapeutic. Education typically involves information about the cyclical nature of sleep, perpetuating causes of chronic insomnia and key remedies. Education about sleep is financially and time inexpensive for both practitioners and patients.28
A comprehensive eBook, How to Sleep Better, has been developed to assist GPs and patients with education and is freely available (see Box8,29-31). Although the efficacy of education as a standalone treatment for insomnia is inferior to that of more comprehensive treatment methods, such as CBTi, its relative efficacy when compared with the other methods more suitable for deployment in general practice is unknown.
{kind=link}
Digital CBTi
With the rise in popularity of technology and portable devices, a range of digital sleep improvement programs have been developed, which may be suitable for use in general practice. These programs are delivered via the internet and mobile devices, whereby the user participates in four to six interactive weekly sessions. The efficacy of these programs relative to credible placebo programs of similar duration has been shown, with the magnitude of reductions in insomnia symptoms akin to those observed after CBTi delivered in person.32-34 The ease of accessibility of digital programs promotes CBTi-based treatment throughout the community.
Although the most widely investigated digital CBTi programs (Sleepio and SHUTi) are not currently available in Australia, other digital programs based on the same CBTi evidence and strategies are available (see Box). Digital CBTi programs are highly effective among patients who complete the full four- to six-week course, but about 40 to 60% of patients do not complete the full program. These patients may either require motivational support or contact to encourage adherence or may be more suitable for a face-to-face CBTi option.35
CBTi administered in general practice
CBTi is the gold-standard treatment for insomnia and has great potential for insomnia management in general practice. Although CBTi produces robust and durable improvements in sleep, it is traditionally administered over six to 12 weeks on an individual basis, with consultations varying from 15 to 50 minutes. This limits its feasibility for use in general practice, particularly given the significant time and financial costs for both the patient and clinician.36
A step-by-step approach for GPs to manage insomnia using a brief CBTi program, tailored to the Australian general practice time and funding model, has recently been developed.29 Our group has also shown the clinical efficacy of a brief, group-based treatment program, conducted over four weekly sessions, whereby improvements in sleep and daytime functioning were notably superior to those of some longer, one-on-one programs.21,24,37 This program is the shortest face-to-face CBTi program to date, and the standardised nature of the treatment program ensures effective administration by individuals who are not extensively trained. This program is ideally suited for administration by upskilled GPs, practice nurses or other healthcare workers (an important component to ensure delivery to rural and remote patients who are unable to access intensive clinical services).
Referral to a psychologist for CBTi
Referral to a psychologist who specialises in CBTi is best practice for insomnia management.38 The Australian Psychological Society ‘Find a Psychologist’ search tool may be used to find local psychologists who specialise in CBTi and the management of insomnia (see Box).
Sedative-hypnotic withdrawal
Sedative-hypnotic medications increase sleep time initially but are associated with increasing risks of cognitive and psychomotor side effects, serious adverse events, patterns of long-term dependence and mortality when used for longer periods.8,39-41 Furthermore, the rapid development of pharmacological tolerance results in reduced effectiveness and a tendency for dose escalation, while attempts to reduce the dose lead to rapid onset of withdrawal and rebound symptoms.8,40 Many patients with insomnia managed in general practice may require support in withdrawing from sedative-hypnotic medications. Gradual withdrawal from these medications may reduce withdrawal or rebound symptoms, and NPS MedicineWise has developed a gradual withdrawal plan to assist with this (see Box).8
CBTi facilitates successful withdrawal from sedative-hypnotic medications in general practice patients.42,43 For example, CBTi may facilitate withdrawal by reducing withdrawal or rebound symptoms that often complicate the withdrawal process, providing patients with the initial confidence to withdraw from sedative-hypnotics, or resulting in sustained reduction in insomnia after withdrawal to help prevent relapse of sedative-hypnotic use. A recent review of 95 studies including over 10,000 patients supports the use of digital, nurse-administered and psychologist-administered CBTi strategies in facilitating sedative-hypnotic withdrawal.44 CBTi may be initiated in combination with sedative-hypnotic medications, to improve sleep and prevent rebound or withdrawal symptoms, as patients are provided with support to gradually reduce medication use over the course of several weeks.
Research opportunity
The translation of best-practice management of insomnia to the general practice setting is the basis of an NHMRC-funded National Centre for Sleep Health Services Research Excellence program: Positioning Primary Care at the Centre of Sleep Health Management (2018–2022). GPs who are interested in becoming involved in this research program or in research outputs from the program, or who would like to contribute any feedback on this article or experiences from their own practice, are invited to contact the authors at www.ncshsr.com/contact.
Conclusion
As the most common sleep disorder and one with significant associated health risks, reduced quality of life and economic burden, insomnia is problematic for general practice. Pharmacotherapy continues to be the default treatment because it is simple, quick and can be prescribed in the most common 15-minute consultations. However, its limited symptomatic relief rarely provides long-term remission, and it is associated with significant adverse side effects, including drug dependence. RACGP guidelines have recognised this problem and recommend the use of CBTi as first-line treatment, instead of drugs.8
Many GPs also recognise the need for effective nondrug therapies but lack the training and time needed to administer CBTi.36 However, there are a variety of CBTi options, ranging in cost, availability and evidence-based effectiveness, that can be used by GPs. These include sources of useful educational information about sleep and insomnia, online or digital CBTi programs, brief behavioural therapies that can be administered in general practice settings and referral pathways to registered psychologists experienced in CBTi. MT