Rabies immunisation: update for travellers

Rabies is a zoonotic disease prevalent throughout the world, particularly in underdeveloped countries. Although Australia is rabies-free, rabies-like lyssaviruses carried by bats pose a risk of infection. Australians travelling to and arriving from rabies-prone areas are also at risk of contracting rabies. Pre- and postexposure rabies immunisations are available in Australia and GPs should recommend these when indicated, and advise animal avoidance while travelling overseas.
Rabies is a fatal acute progressive encephalomyelitis that causes nearly 60,000 human deaths per year, mainly in resource-poor countries, due to a lack of awareness and access to safe and effective rabies vaccines and immunoglobulins. However, death from rabies is readily preventable with animal avoidance and proper pre-exposure management, and postexposure immunisation substantially enhances survival (Box 11,2).
{kind=link}
This article focuses on immunisation for those travelling or returning from overseas and should be read in conjunction with, and with reference to the chapter on rabies and other lyssaviruses in the Australian Immunisation Handbook (AIH).3
Rabies virus taxonomy and properties
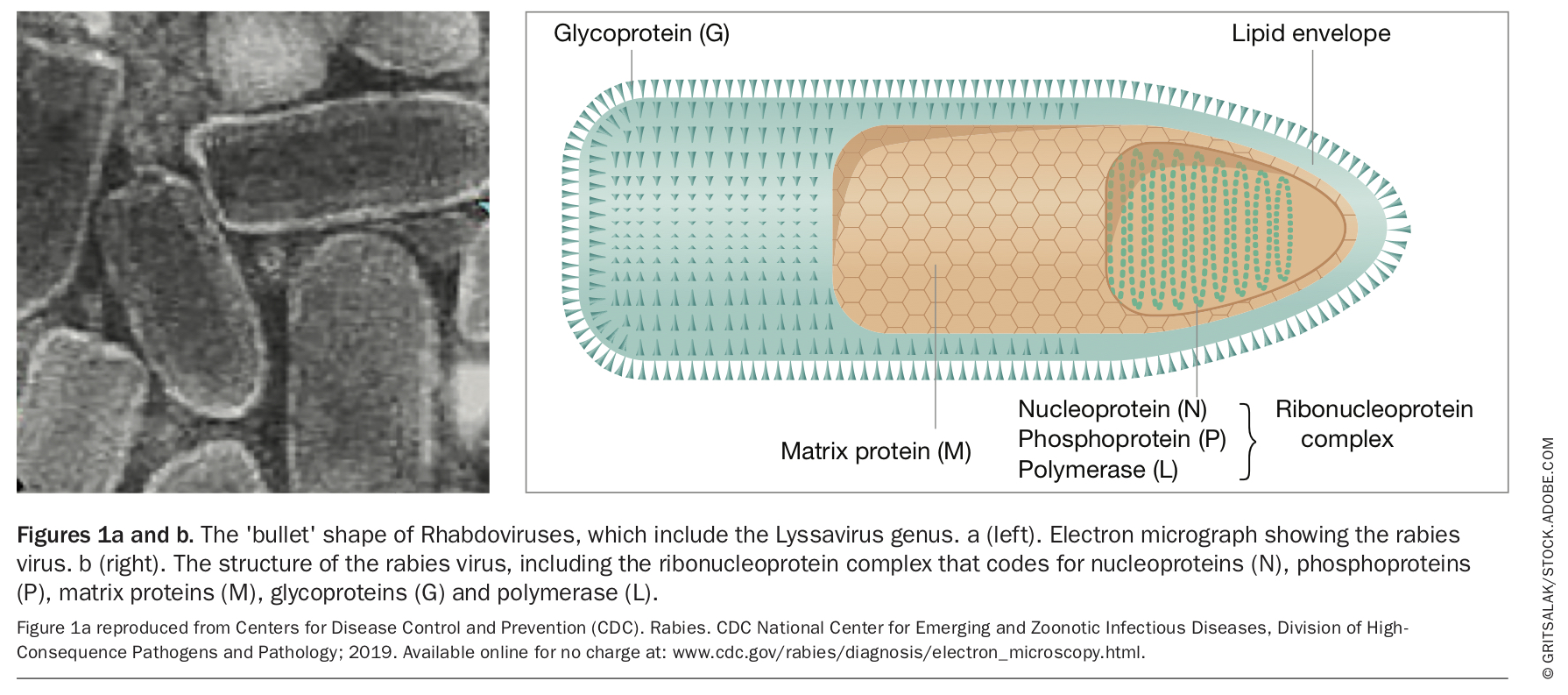
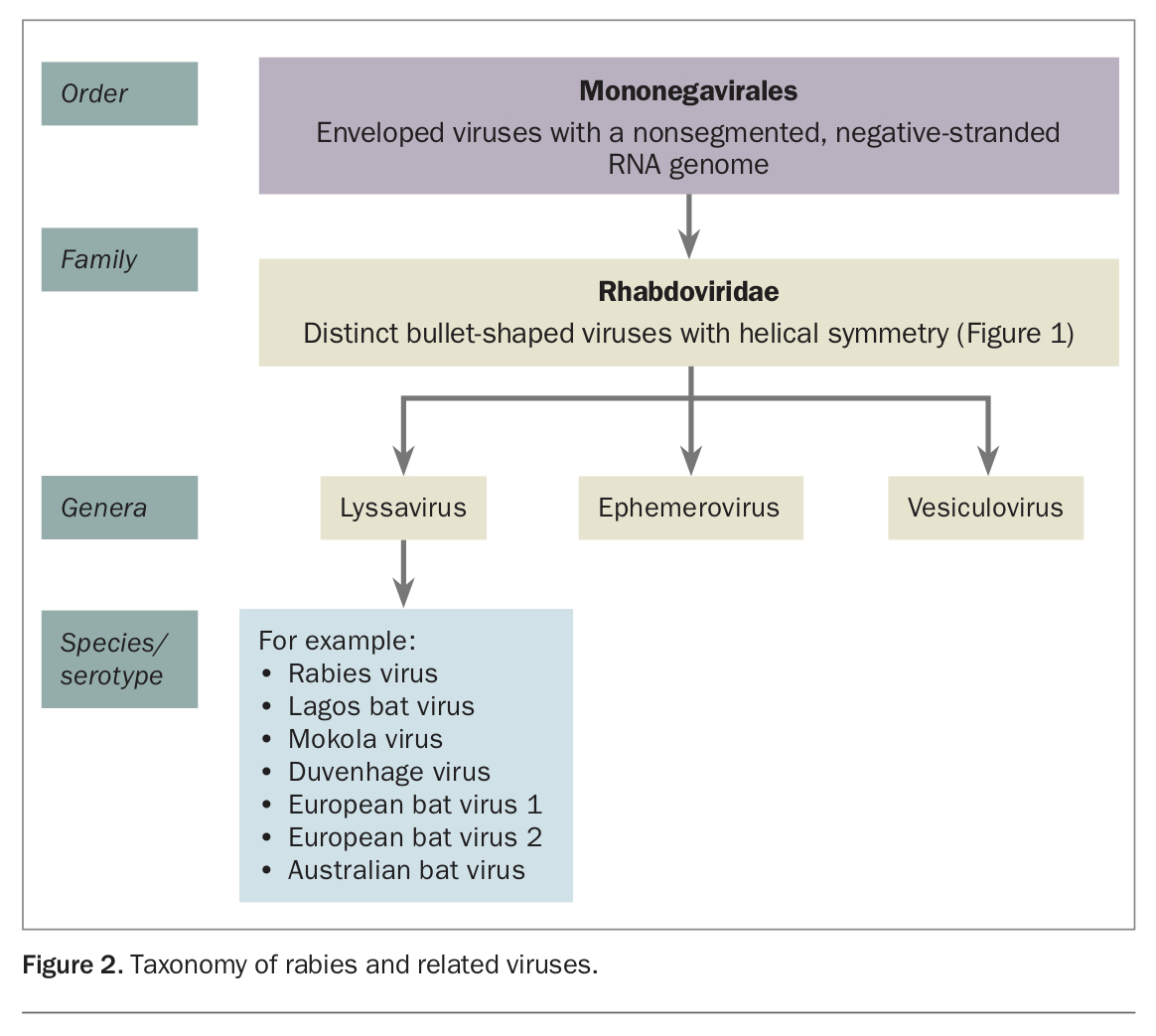
Rabies is derived from the Latin word rabere (to rage). Rabies virus (RABV) belongs to the order Mononegavirales, which are enveloped viruses with a nonsegmented, negative-stranded RNA genome. It is part of the distinctly bullet-shaped Lyssavirus genus (Figures 1a and b), which also includes the serotypes Lagos bat virus, Mokola virus, Duvenhage virus, European bat virus 1 and 2 and Australian bat virus (Figure 2).4 Lyssaviruses cause acute progressive fatal encephalomyelitis. The negatively stranded RNA codes for 5 proteins: nucleoprotein, phosphoprotein, matrix protein, glycoprotein and polymerase. The glycoprotein is the only viral protein exposed on the surface of the virus and is not only the major determinant of viral pathogenicity, but also the major protective antigen responsible for inducing protective immunity against rabies by eliciting virus-neutralising antibodies.5,6
{kind=link}
{kind=link}
There are few viruses as successful as RABV; it has survived for millennia (over 4000 years) in most parts of the world.7,8 There are a wide range of hosts for the virus. It can replicate in all warm-blooded animals, where the resultant disease is almost invariably fatal. The virus ensures its own survival by influencing the behaviour of the afflicted host in ways that lead to virus transmission; rabid animals often behave aggressively, attacking humans and other animals without provocation.8
RABV infectivity is destroyed by lipid solvents, hence cleansing and sterilising wounds is an essential part of postexposure prophylaxis (PEP). RABV cannot survive for long periods in the environment, except in a cool dark area, and is susceptible to ultraviolet radiation or heat of one hour at 50°C and rapidly inactivated in sunlight.9 Rabies virus becomes noninfectious when it dries out, or when it is exposed to sunlight.10 So in general, if the material containing the virus is dry, it can be considered noninfectious.
Rabies virus transmission and pathogenesis
RABV is transmitted mainly through direct contact (such as through broken skin or mucous membranes in the eyes, nose or mouth) with saliva or brain/nervous system tissue from an infected animal. People usually get rabies from the bite of a rabid animal. Such an animal is generally a mammal that may attack humans and transfer saliva. Among laboratory workers and cave explorers, RABV may be transmitted through inhalation of aerosolised virus, although this is uncommon. Transmission occurs rarely from nonbite exposures such as scratches, abrasions or open wounds that are exposed to saliva or other potentially infectious material from a rabid animal.10 In the cases outlined in Box 2, doctors did not consider rabies as a possible diagnosis, and the consequences to the patient were fatal.11,12 These cases highlight the need for GPs to be vigilant when assessing patients who have returned from overseas travel, especially from countries where rabies is endemic.
{kind=link}
Human-to-human transmission of RABV is extremely rare, apart from transmission through corneal and solid organ transplants. There was a single report of likely perinatal transmission.13 No cases of human rabies resulting from consumption of raw meat or milk from a rabid animal have been reported.13 RABV infection of rodents is very uncommon and no human rabies case from rodent exposure has been documented.13
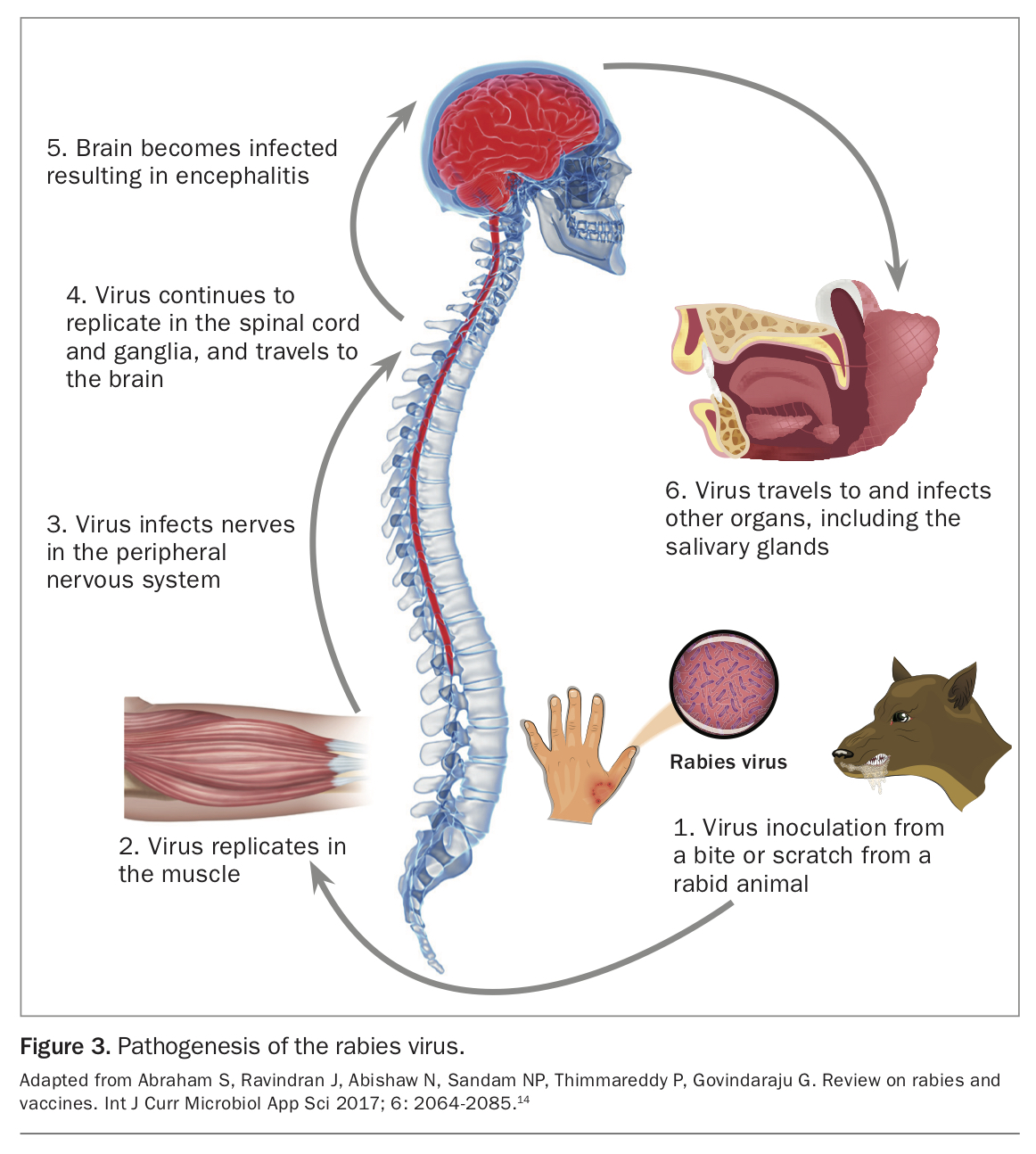
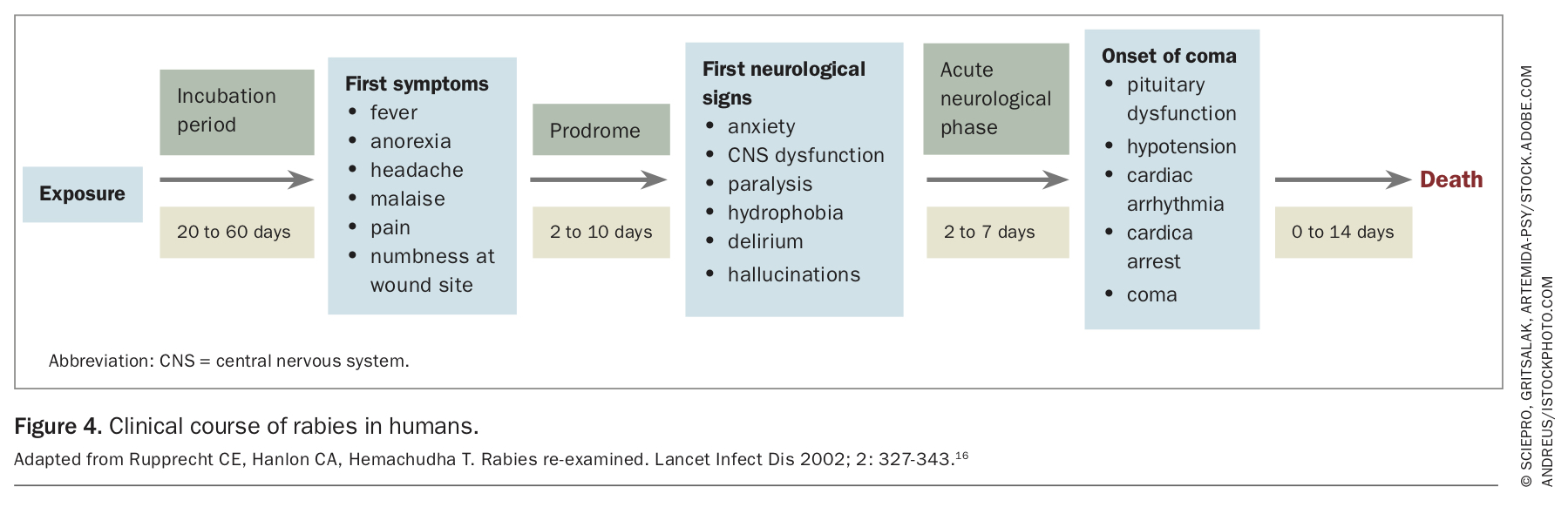
RABV infects the brain and leads to encephalitis. The virus also infects most other organs, especially salivary glands, skin, mucosal surfaces and the gut (Figure 314). The incubation period varies with the amount of virus transmitted, the virus strain, site of inoculation (bites closer to the head have a shorter incubation period), pre-existing host immunity and nature of the wound.15 The incubation period may last for weeks to months before symptoms manifest (Figure 416),17 although longer incubation periods of up to six years have been reported.18
{kind=link}
{kind=link}
Global burden of rabies
According to the Centers for Disease Control and Prevention (CDC), rabies occurs globally and causes more deaths in humans than any other zoonotic disease, and almost all cases of rabies in humans (99%) are dog-mediated.13,19 The reported number of deaths from rabies in humans is often an underestimate of the true burden of disease because of under-reporting.
Rabies from exposure to bats
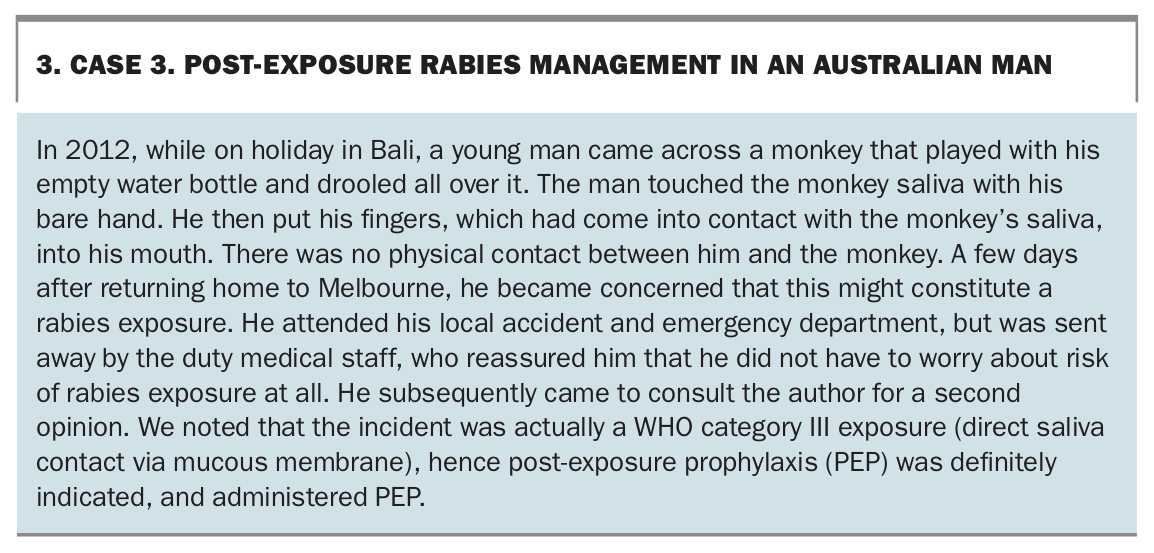
There are a range of animal vectors that can transmit RABV including cats (Box 2, Case 2) monkeys (Box 3, Case 3) and most notably, bats. Bats anywhere in the world are a potential source of lyssaviruses and a potential risk for infecting humans with rabies. In the UK, the Daubenton’s bat species can carry a variation of rabies called European bat lyssavirus 2 (EBLV-2).20,21 In 2002, a bat handler who had not travelled outside the UK died from bat rabies caused by EBLV-2. Only three other human cases of EBLV infection (all fatal) have been reported in Europe in the past 30 years.1
{kind=link}
In recent years in the US, bats surpassed raccoons as the animal most likely to carry rabies. Among 125 human rabies cases reported between 1960 and 2018, 89 were US acquired, including six from organ transplantations, 36 (28%) from dog bites during international travel and 62 (70%) attributed to bats.22 Since 2000, vampire bats have been the leading cause of human rabies in Latin America and the Caribbean.23
Rabies in Australia
Australia is listed as being free of the rabies virus in land dwelling animals. However, the Australian bat lyssavirus (ABLV), which is closely related to RABV, does occur in Australia, and can be transmitted from bats to humans. Bat lyssaviruses are spread the same way as RABV, and like rabies, are usually fatal once symptoms develop.3 There is evidence of ABLV infection in all four species of Australian fruit bats (flying foxes) and in several species of Australian insectivorous bats (Figure 524).3,25
{kind=link}
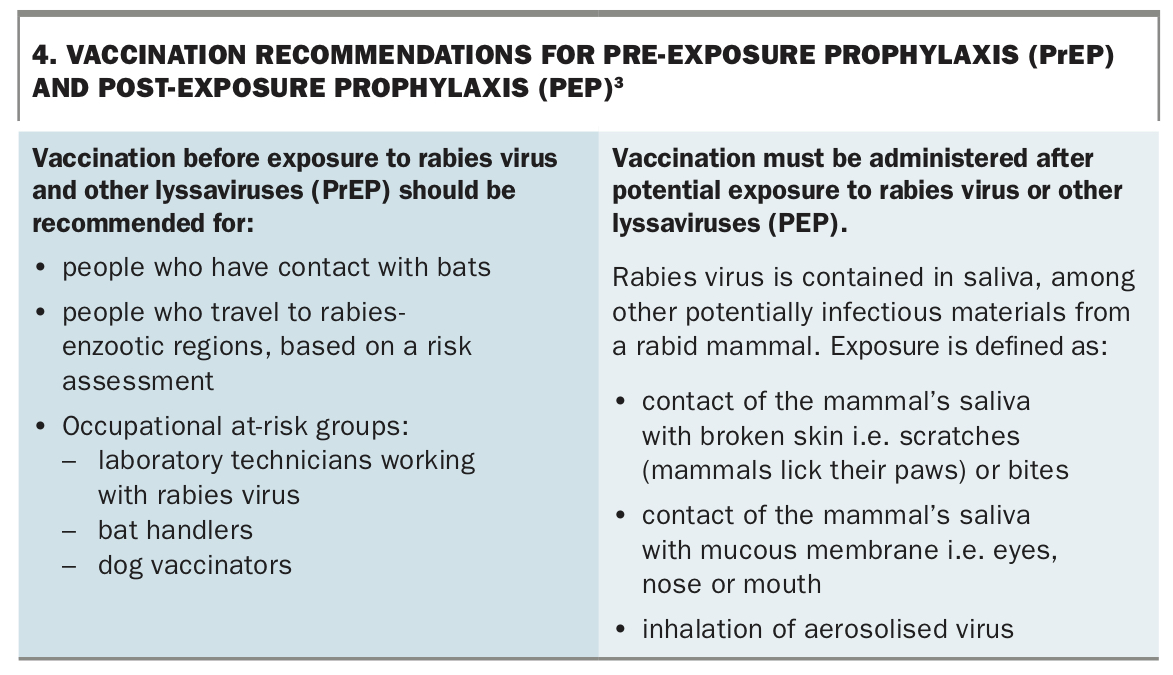
Three cases of human infection with ABLV have been recorded since the virus was first identified in Australia in 1996. All cases were in Queensland and occurred after people were bitten or scratched by bats – and all three people died as a result of ABLV infection.26,27 In Australia, there have been two confirmed human deaths from RABV, in 1987 and 1990.28,29 In both cases, the infection was contracted overseas. Although Australia is rabies free, it is important that Australian GPs are able to provide up-to-date advice on the risk of rabies to patients travelling overseas, recommend pre-exposure prophylaxis (PrEP) whenever indicated, and consider rabies as a possible diagnosis in relevant cases (Box 43).
{kind=link}
Rabies vaccines and immunoglobulins
Rabies immunisation available globally
The first rabies vaccine was developed and successfully administered by Louis Pasteur in 1885. These nerve tissue-derived vaccines were only used for PEP and administered intra-abdominally. Since 1984, the WHO has strongly recommended against the production and use of nerve tissue rabies vaccines, although such vaccines are still used in some developing countries. Despite their comparatively low cost, they are antigenically less potent than the cell culture and embryonated egg-based rabies vaccines (CCEEVs), and appreciably more prone to causing adverse reactions.30
The WHO-approved rabies vaccines are known as either CCEEVs or purified cell culture derived vaccines (CCDVs). These vaccines are safe, highly immunogenic and well tolerated.30
WHO approved CCEEVs or CCDVs include:
- human diploid cell vaccine (HDCV, Merieux)
- purified chick embryo cell vaccine (PCEC, Rabipur)
- purified vero cell rabies vaccine (PVRV, Verorab)
- purified duck embryo vaccine (PDEV, Lyssavac)
All of these are inactivated vaccines, with a minimal acceptable potency of at least 2.5 IU/dose per intramuscular (IM) dose (0.5 mL or 1 mL depending on the brand). Generally, the shelf-life of these vaccines is three years, provided they are stored at 2 to 8°C and protected from sunlight. They may be used interchangeably if absolutely necessary.31
The modern rabies vaccines are generally available in major urban centres of most countries of the developing world.22 However, there are cyclical shortages internationally and in Australia.32-34 Rabies immunoglobulin (RIG) is in short supply in many countries with rabies-infected dogs and may not be available, even in major urban centres.32 There are recent confirmed reports of poor quality or counterfeit products available in China and the Philippines.35,36
Rabies immunisation available in Australia
Merieux HDCV and Rabipur PCEC are available in Australia. However, in view of recent shortages of these vaccines, the TGA has approved the use of Verorab PVRV, being made available under the special access scheme as an interim measure.
In Australia, PEP is supplied free of charge by state and territory health authorities, via the Accident and Emergency Departments of local teaching and district hospitals, as well as some travel clinics. In cases of suspected rabies exposure, PEP is indicated regardless of time since exposure. PrEP consisting of three full IM or subcutaneous (SC) doses of a CCDV is recommended for those who are at risk of contracting rabies or coming into contact with animals carrying the virus (Box 5).
{kind=link}
Updated recommendations on rabies immunisation
The Strategic Advisory Group of Experts (SAGE) on Immunization, a part of the WHO, recently issued recommendations on rabies PrEP, PEP and RIG administration (Box 6).30,37,38 Their recommendations aim to maximise use of resources and enhance compliance, particularly in low- income countries, which bear the highest disease burden of rabies.
{kind=link}
Updates to PrEP recommendations
The latest WHO position paper on rabies vaccine has incorporated the SAGE recommendations.39 There has been precedent for reducing rabies immunoprophylaxis recommendations in favour of the abbreviated rabies PrEP on days 0 and 7. When CCDVs first appeared in the 1970s, PEP consisted of six doses, given on Days 0, 3, 7, 14, 28 and 90. The sixth dose was dropped in the 1980s, and the fifth dose was dropped by US authorities (during a rabies vaccine shortage) in the 2000s. Australian health authorities adopted this modified four-dose Essen PEP regimen in 2011. Booster dose recommendations were also changed from booster-only for those at risk instead of every two years. Boosters are no longer recommended in people who have only intermittent risk of rabies exposure. To date, there has not been any increase in deaths from rabies as a result of these modifications.40 As repeatedly shown, neither the number of previous PrEP doses nor the mode of application significantly influences the speed of an adequate immune response.2,38
The conventional three-dose PrEP schedule (on days 0, 7 and 21 to 28, i.e. Essen regimen) is still recommended for the clinically immunocompromised, those aged over 65 years (because of paucity of data), and those in occupational at-risk groups including laboratory technicians working with RABV, bat handlers and dog vaccinators.38
The Australian Department of Health, CDC, and UK National Travel Health Network and Centre have not changed their national recommendation on PrEP and continue to endorse the conventional Essen regime, recommending a (full-dose) IM/SC route instead of a (low-dose) intradermal (ID) route.2,41,42 The use of ID rabies vaccination is considered off-label and there are no available data on whether ID rabies vaccination protects against infection with other lyssaviruses such as ABVL.3
Updates to PEP and RIG recommendations
The other major change in the WHO recommendations is on the use of RIG in rabies PEP. RIG dose should be infiltrated into and around the wound as much as anatomically feasible. The remaining RIG dose should not be administered into a site distant to the wound (i.e. gluteal region), it should instead be conserved for other patients.39 Tetanus vaccine must also be given when indicated.
Primary PEP failures are extremely rare. Around 20 million PEP treatments are given globally each year. Failures are mostly notified in developed countries and under-reported in developing nations. The principal identified causes of PEP failure involve deviation from protocol and include:31
- delay in seeking rabies prophylaxis
- lack or improper administration of RIG (e.g. failure to inject all bite sites)
- lack of or improper primary wound care
- poor-quality rabies vaccine
- bites in highly innervated regions of the body such as hands and face.
At the time of writing, Australian health authorities have not formally taken up any of the latest WHO recommendations on rabies immunisation. Health practitioners should follow the AIH for guidance in the management of rabies.3
Conclusion
There is an alarming lack of awareness of the risk of rabies globally, particularly among front-line healthcare workers in affluent countries that have been free of rabies for decades. Rabies is fatal if left untreated; however, death from rabies is preventable with PEP including prompt, thorough wound cleansing and sterilisation, and administration of CCDV and human RIG if indicated. Australian GPs need to be vigilant in informing patients who are travelling or who have returned from overseas of the risk of contracting rabies and to recommend PrEP and PEP as needed. Travel medicine practitioners must be proactive in strongly advising animal avoidance and advocating PrEP whenever indicated. MT
References
attachment_data/file/723607/GreenBook_chapter_27_rabies.pdf (accessed February 2020).
734195/PHE_Vaccine_Update_282_August_2018_.pdf (accessed February 2020).
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.