Managing depression using a clinical practice guideline approach

The 2020 update of the Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders provides a new framework for managing depressive disorders that moves beyond the stepped care approach. This framework is based around three key components: actions, such as lifestyle modification and patient education; choices in pharmacological treatment that include the patient’s preferences; and potential alternative treatments.
- Attending to lifestyle factors (sleep hygiene, diet, exercise and alcohol and substance misuse) is a necessary first step in the management of major depression.
- Psychological treatments, such as cognitive behaviour therapy (CBT), interpersonal psychotherapy and problem solving therapy, are recommended for all patients with depression.
- Digital (online) therapies and therapies delivered via telehealth are efficacious and should be offered to those who are unable to access face-to-face therapy.
- Advantages of digital therapies include accessibility, convenience and fidelity to the treatment model (usually CBT). However, these treatments are not suited to everyone.
- Choice of antidepressant medications requires a balance of efficacy with tolerability and can be guided by the patient’s symptom profile.
- Electroconvulsive therapy is the treatment of choice for people with severe depression and those who do not respond to antidepressant medications.
Clinical practice changes and evolves over time in response to new findings from research and environmental changes, as exemplified by the COVID-19 pandemic. Clinical practice guidelines should reflect such changes and, accordingly, the Royal Australian and New Zealand College of Psychiatrists updated its 2015 clinical practice guidelines on mood disorders (MDcpg2015) in 2020 (MDcpg2020).1,2 These updated guidelines take a new approach to the management of mood disorders, moving beyond a stepped care approach.
Key changes to the guidelines are an increased emphasis on essential ‘actions’ that need to be taken in the management of depression. These ‘actions’ focus on promoting a healthy lifestyle and encourage focused psychological treatments. The guidelines are also innovative in their approach to selecting ‘choice’ pharmacological treatments and reacting to a suboptimal response. For this, the guidelines introduce a new paradigm – the MIDAS (medication, increase dose, augmentation, switch) approach. The guidelines also break ground as they discuss in detail antidepressant withdrawal and how to manage withdrawal symptoms. Further, they position treatment ‘alternatives’, including electroconvulsive therapy (ECT), repetitive transcranial magnetic stimulation (rTMS) and novel treatments such as esketamine, according to the evidence that is available when choice treatments are not effective. This article describes the approach of the new MDcpg2020 for a broader audience. It considers the key evidence- and consensus-based recommendations for the management of major depression.
Overview of depression
Major depression is a common disorder, with a 12-month prevalence of 6%, and with up to 18% of individuals experiencing an episode of major depression in their lifetime. Importantly, it is more common in women than men, a fact that distinguishes it from bipolar disorder, and it is prominent in primary care presentations, where most of its management takes place.
Typically, episodes of acute depression last several months and full recovery can take up to a year; however, it can sometimes take much longer. Depression is often a recurrent disorder, with up to 80% of patients experiencing further episodes in their lifetime.3 It is also episodic, and about 50% of those affected by a major depressive episode recover within six months, increasing to nearly 75% within a year. Nevertheless, over a quarter remain unwell and develop a chronic depressive disorder.
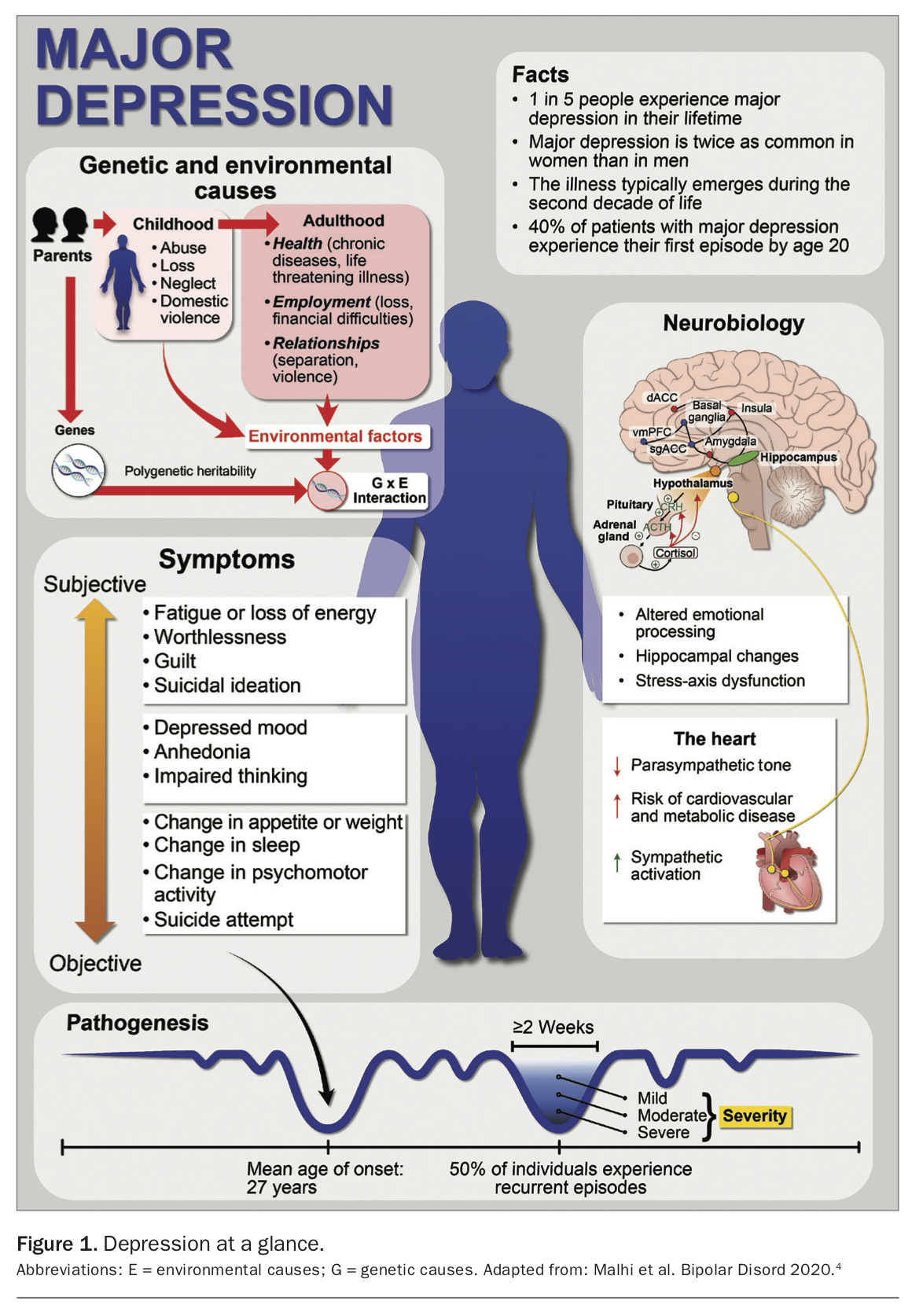
The origins of depression are covered in considerable detail in the MDcpg2020, with detailed explanations of stress models and circadian function that are known to contribute to the aetiology of depressive disorders (Figure 1).2,4 Detailed discussion of these matters is beyond the scope of this article, which focuses on the management of depression.
{kind=link}
Diagnosis and formulation
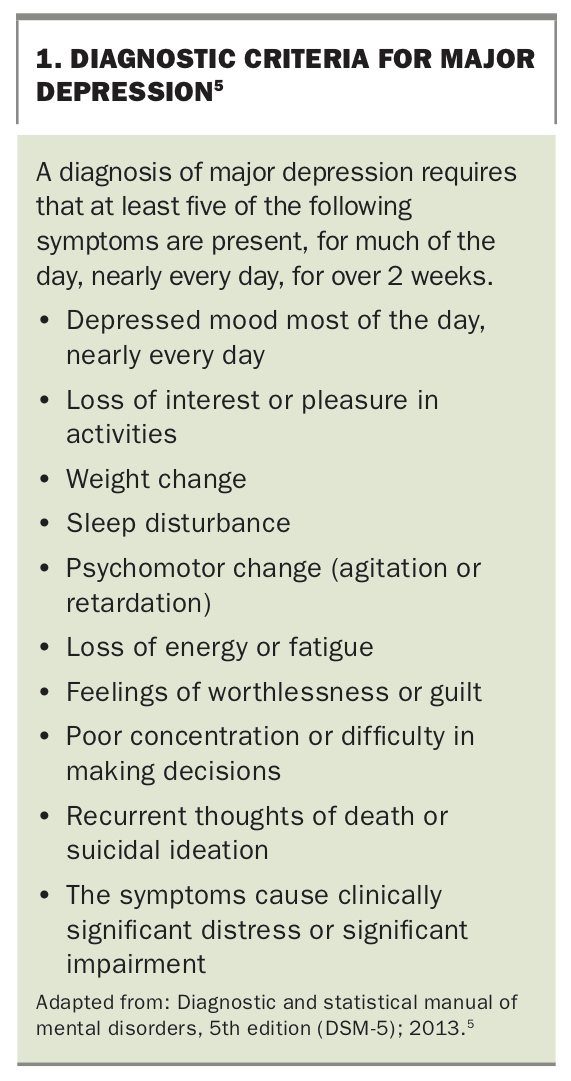
Akin to its predecessor, the MDcpg2020 emphasises the importance of making a clear diagnosis from the outset, as this serves as a starting point for management. Distinguishing patients who present with transient depressive symptoms (that might arise though current life stressors, such as having to cope with COVID-19 lockdowns) from those with an episode of major depression, characterised by persistence of five or more symptoms for over two weeks, is key (Box 1).5
{kind=link}
It is also important to distinguish between patients with bipolar depression and a depressive episode and those with unipolar major depression. The management approach for patients with bipolar depression prioritises mood stabilisers, as antidepressants can trigger a manic episode in such patients. Diagnosis is straightforward for patients with established bipolar disorder but is difficult for those with a first episode of depression as the symptom patterns are similar. A family history of bipolar disorder and previous mild manic episodes should raise a high index of suspicion for possible bipolar disorder. The management of bipolar depression is beyond the scope of this article, but is discussed in detail in the MDcpg2020.
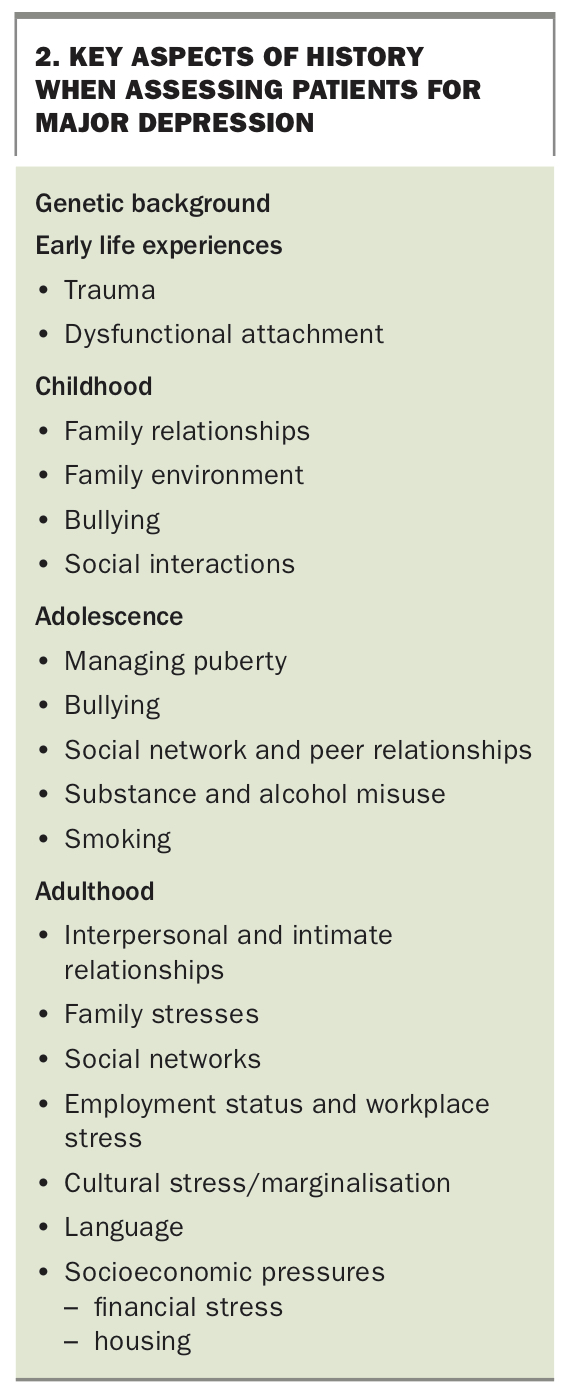
Although establishing that the patient meets criteria for major depression is important, it is equally crucial to make sense of the depressive illness. Understanding the nature of the illness, its context, origins and emergence is pivotal to devising a management plan and involves ‘formulating’ the patient’s depressive episode. Such a formulation involves plotting the course of the depressive episode and identifying its triggers and maintaining factors. It also involves identifying the underlying developmental factors, such as early life trauma, childhood factors, family and current interpersonal relationships, support networks and lifestyle factors, that interact with each other contributing to depression vulnerability (Box 2). Formulating the episode is discussed in detail in the MDcpg2015 and the MDcpg2020.
{kind=link}
Managing depression
The framework for managing depression outlined in the MDcpg2020 consists of three components aimed at achieving complete remission (Figure 2). The foundations of good management require certain ‘actions’ that must be instituted whenever possible. These include lifestyle changes and psychological interventions. If remission has not been achieved using these actions, pharmacotherapy with antidepressant ‘choices’ is recommended, and should be trialled initially. These antidepressant choices can also be used as part of more complex regimens involving combinations of pharmacotherapies and other treatment strategies. Finally, if there is still no response, a number of ‘alternatives’, including complex medication strategies and physical treatments such as ECT, can be used. These are generally in the province of specialist care.
{kind=link}
Psychoeducation
Providing the patient and ‘significant others’ with information about depression is essential. In the first instance, this should address the depressive symptoms they are experiencing, likely contributing lifestyle factors and the various available treatment options. More extensive psycho-education should be provided to the patient and carer according to the stage in management and patient understanding, and should include:
- more detail about the nature of depression and likely outcome of treatment
- coping and self-management strategies
- the need to manage work-life balance
- managing pharmacotherapy (if implemented) and side effects
- how to identify early warning signs of depression.
Lifestyle modification
Lifestyle factors, in particular poor diet, poor sleep patterns and lack of exercise, it can play a role in the onset and maintenance of an episode of depression.6 Encouraging the patient to adopt a healthier lifestyle, while acknowledging that this is a challenging task, is foundational in the management of a depressive episode. A healthier lifestyle can significantly reduce the severity of depression in addition to having wider health benefits. Specifically, a poor diet is associated with depression, and transition to a healthier diet, such as the Mediterranean diet, characterised by high vegetable, fruit, fish and grain components and low animal fat, has been shown to reduce depressive symptoms.7,8
Although sleep disturbance is a common and key symptom of depression (initial or terminal insomnia or hypersomnia), it can also contribute to the onset of depression and its maintenance. Implementing healthy sleep hygiene is foundational in managing depression, with patients encouraged to follow the basic principles of sleep hygiene: instituting a regular bedtime and wakeup time, avoiding overstimulation (including stimulant drinks) before going to bed, not using phones or tablets (the blue light suppresses melatonin production) or watching TV in bed, and getting up time. Patients can be directed to good quality information (e.g. www.sleepfoundation.org/articles/sleep-hygiene) or an app to record sleep information (such as CBT-i Coach).
Regular exercise is associated with improved quality of life and has been shown to have significant antidepressant effects in people with depression.9 Therefore, exercise – particularly aerobic exercise – should be encouraged in all patients, not least because of its general health benefits.10
Modifying unhealthy behaviours
Addressing unhealthy lifestyle habits that may be contributing to depression, such as excessive alcohol intake and substance misuse, is important. The relationship between alcohol misuse and depression is complex; however, encouraging patients to reduce alcohol intake is crucial to managing depression (see NHMRC recommendations for more detail).11 Referral to an addiction service is sometimes necessary, especially when alcohol dependence is suspected. Similarly, substance misuse needs to be promptly and properly addressed as illicit drugs will interfere with recovery. When this is problematic, referral to an addiction service may be needed. Smoking is associated with depression, and cessation is strongly encouraged to allow for full recovery.12 Furthermore, smoking cessation clearly has significant benefits for the individual’s general health.
Psychological treatments
The MDcpg2020 recommends psychological treatments for all patients presenting with depression. Although cognitive behaviour therapy (CBT) is probably the most familiar form of psychological treatment, other effective structured psychological treatments include interpersonal psychotherapy (IPT), problem solving therapy, behavioural activation therapy, short-term psychodynamic therapy and nondirective supportive therapy. Equivalent efficacy of psychological treatment to antidepressant medication has been shown for patients with mild to moderate depression.13 However, such findings need to take into account the types of patients recruited into the studies and the ‘control’ intervention (often wait list groups) that may favour the active treatment.
Psychological interventions are generally preferred by patients and have fewer adverse effects, although possible ‘side effects’ include resurfacing of unpleasant memories, difficulties in interpersonal relationships and demoralisation with slow progress.14 However, psychological interventions can help patients develop strategies for dealing with adversity and transient mood changes, which builds towards developing resilience and relapse prevention.
When referring patients for psychological treatment, important considerations include access and the selection of an appropriate therapist. Taking into account patient preference is also important as treatment outcomes are usually better if patients get their preferred treatment, particularly when the choice is between psychological and pharmacological treatments.15 If a patient has a clear preference for medication, referral to a psychologist may be fruitless, although the benefits of such a referral should be pointed out and the patient may consider psychological treatment later in the course of their illness, for instance when in remission. When the patient does not have a clear preference, the pros (antidepressant efficacy and changes in quality of life) and cons (side effects, costs, inconvenience and likelihood of relapse) of each treatment option should be explained to the patient as part of a shared decision making process. The advantages of combined treatment (pharmacotherapy and psychotherapy) should be emphasised, particularly its value in relapse prevention.
A good ‘fit’ between therapist and patient is more likely to achieve the optimal outcome of psychological treatment. Identifying a therapist who the patient can work with and who has appropriate qualifications and training in an evidence based approach is important. The therapist should adhere to the selected treatment model (e.g. CBT), as consistency in treatment with one model is most effective. Insufficient evidence exists to predict which patients would benefit from a specific form of therapy (i.e. which patient will respond to CBT versus IPT). Although these considerations are important, in practice, the choice of therapist usually depends on local resources and availability.
Perhaps the most important consideration is access to psychological treatments; clearly this is an important issue as disadvantaged, rural and regional areas have limited access to trained psychologists. Access to psychological treatments is now available to all through either telehealth services (telephone or video), which have expanded during the COVID-19 pandemic, or the internet using ‘digital’ therapies (interventions offered online via computer, tablet or smart phone). CBT provided via telehealth has comparable efficacy to face-to-face CBT and has a clear advantage in providing access to those who are unable to attend face-to-face visits (as shown during COVID) and those living in rural and remote areas.16 However, once again, the major constraint in providing CBT via telehealth is the availability of trained therapists.
Digital therapies (predominantly based on CBT) overcome accessibility problems as a therapist is not needed. Rather the patient is guided through the modules covering the major ingredients of CBT such as psychoeducation, behavioural strategies, challenging dysfunctional thoughts, structured problem solving and relapse prevention. Some programs provide feedback through assessments of symptom severity and require the patient to do homework. Others are therapist guided (with limited access to ‘chat’ to a therapist), which improves the effectiveness of the intervention. Digital therapies have near-equivalent efficacy to face-to-face therapy for depression, with digital CBT having the strongest evidence base. However, research methodology using wait list control groups favours the efficacy of digital interventions and, therefore, further research is needed to determine their true effects. Distinct advantages of digital therapies include:
- accessibility to anyone who has access to a smart phone or the internet
- affordability, with some, such as This Way Up clinic, supported through Medicare
- convenience, as modules can be completed at times that suit the patient
- fidelity to the treatment model (usually CBT), guiding patients through the key ingredients of the approach
- greater acceptability for patients who feel stigmatised by having to see a therapist.
However, digital therapies do not match ‘gold standard’ face-to-face therapy conducted by a skilled therapist and disadvantages include that they:
- do not allow for the flexibility a skilled therapist can provide when dealing with new or emerging patient problems
- are not suitable for ‘technophobic’ individuals or those who may have greater difficulty with working on devices, such as the elderly
- are not helpful for patients who lack motivation (a key problem in those with depression) as they will not engage with the program nor complete all the modules.
- Box 3 provides a list of resources where such programs can be found. Although digital therapies offer immense benefits, these treatments are not suited to everyone.
Pharmacotherapy for depression
A patient who has not achieved remission after lifestyle interventions and psychological therapy and is amenable to pharmacotherapy should be prescribed an antidepressant. In some instances, an antidepressant may be prescribed from the outset, such as when the depression is severe, when prior experience has shown that medication is needed or if the patient has a clear preference for medication.
Patient preference is a key consideration; if the patient is in agreement with treatment, they are more likely to adhere to the treatment regimen. However, a significant proportion of patients will stop their antidepressant for a variety of reasons, including perceived lack of symptom improvement and side effects. Thus, adherence is improved if the patient is involved in the decision about which treatment to take. Typically this should involve a discussion about the expected benefits of the antidepressant and its potential adverse effects. Some adverse effects, such as sedation, may be more acceptable to patients, whereas others, such as weight gain, may be less so. These attitudes are also likely to change over the course of the illness and, therefore, it is a discussion that should be repeated throughout management.
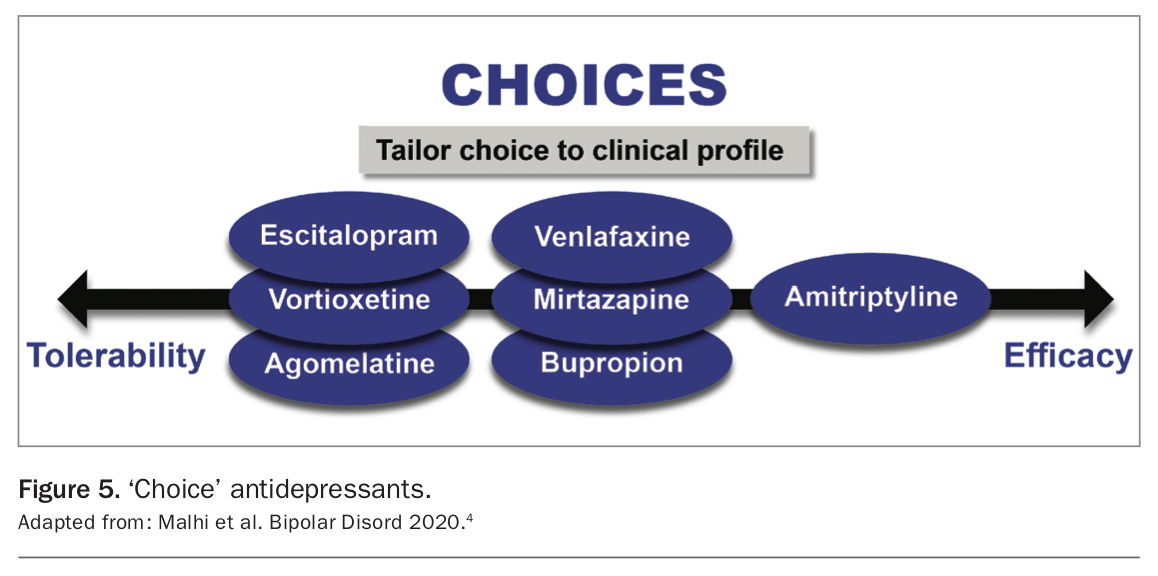
A variety of antidepressants that belong to different pharmacological classes are available. Most act via monoaminergic modulation and differ mainly in their tolerability and only somewhat in their efficacy. Nevertheless, these differences are important and useful for tailoring choice to the clinical profile of the individual with depression. Recent network meta-analyses showed that all antidepressants are effective (compared with placebo) and that some are more effective than others (head-to-head studies).15 Furthermore, many studies have clearly shown that some antidepressants are more tolerable (less side effects) than others. For example, dual-acting antidepressants that target more than one neurotransmitter system, such as the serotonin noradrenaline reuptake inhibitors (SNRIs) and tricyclics, are more efficacious than single-action drugs, such as the selective serotonin reuptake inhibitors (SSRIs)
(e.g. sertraline and escitalopram). However, the more efficacious antidepressants tend to have poorer tolerability.
Overall, when deciding which treatment to prescribe, tolerability is equally as important as efficacy, as most antidepressants require at least one week of administration at an adequate dose before a response is discernible. To achieve this, patients need to take the antidepressant medication every day as prescribed, and the importance of this should be clearly explained to the patient. As medication adherence is crucial from the outset, patients should be asked to be vigilant and monitor for adverse effects of medication in addition to symptom improvement. They should be instructed to report any side effects promptly and to seek assistance and review as soon as possible rather than stopping the medication (unless side effects are intolerable). In practice, a follow-up appointment relatively soon after medication has been commenced is useful (after about two weeks). This also allows for a detailed appraisal of response and a review of overall functioning.
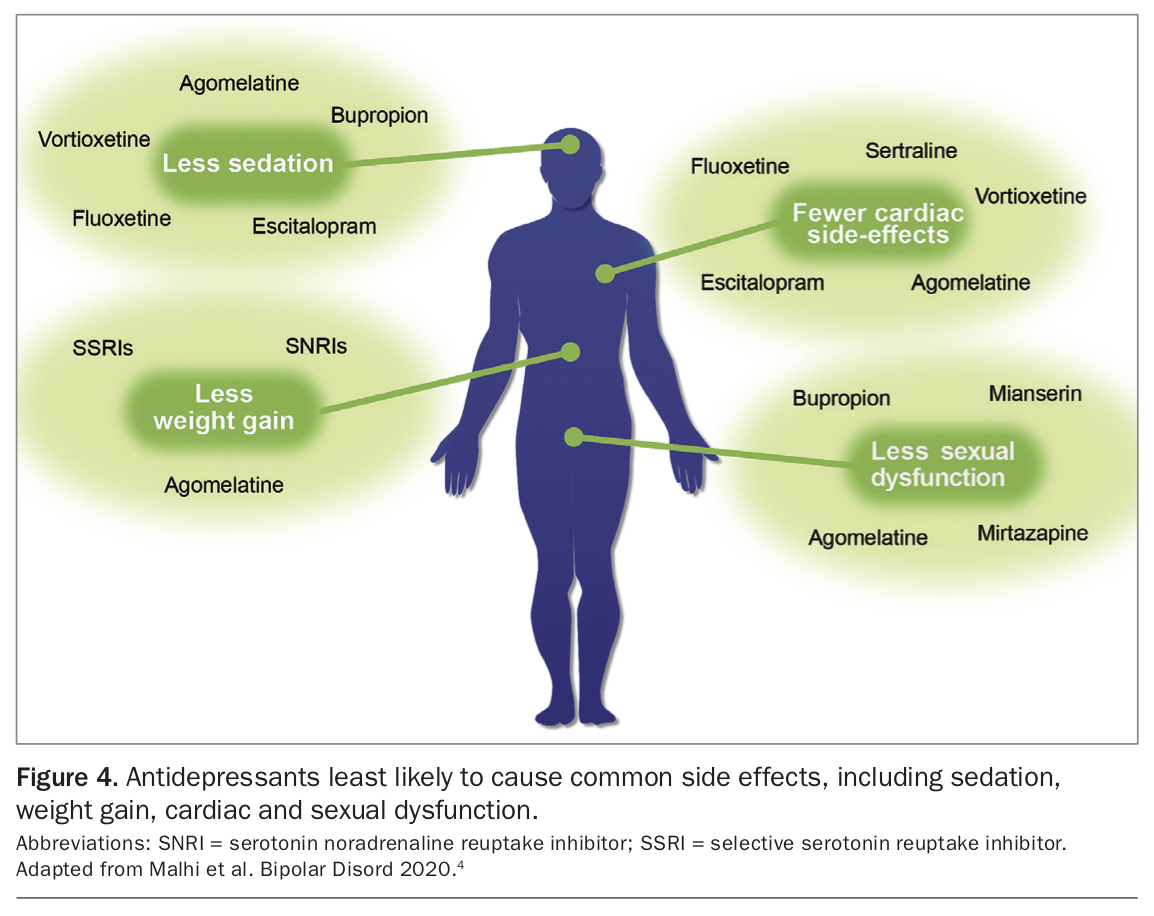
Key side effects that patients often complain of and find most troubling are sedation, sexual dysfunction, weight gain and gastrointestinal symptoms such as nausea and diarrhoea. Considering which side effects the patient is able to manage and which they might find intolerable is important when choosing an antidepressant. Figure 4 provides a simple schematic to identify which anti-depressants are least likely to cause common side effects.4
{kind=link}
Reviewing responsivity and the side-effect profile in patients who have been previously prescribed antidepressants is important, noting in particular the side effects experienced with previous agents. In general, for uncomplicated mild to moderate depression, the initial ‘choice’ antidepressant should be a medication that will be well tolerated and has good efficacy. The ease of switching treatment should be considered as the first antidepressant may not lead to full remission, requiring the patient to change to a different antidepressant.
Collectively, the seven choice agents set out in the guidelines provide a broad range of mechanisms of action (Figure 5).2,4 The monoamine oxidase inhibitors are a notable omission. These have a broad-spectrum of efficacy, but because of their interactions, have been positioned as an alternative antidepressants, rather than a choice agents.
{kind=link}
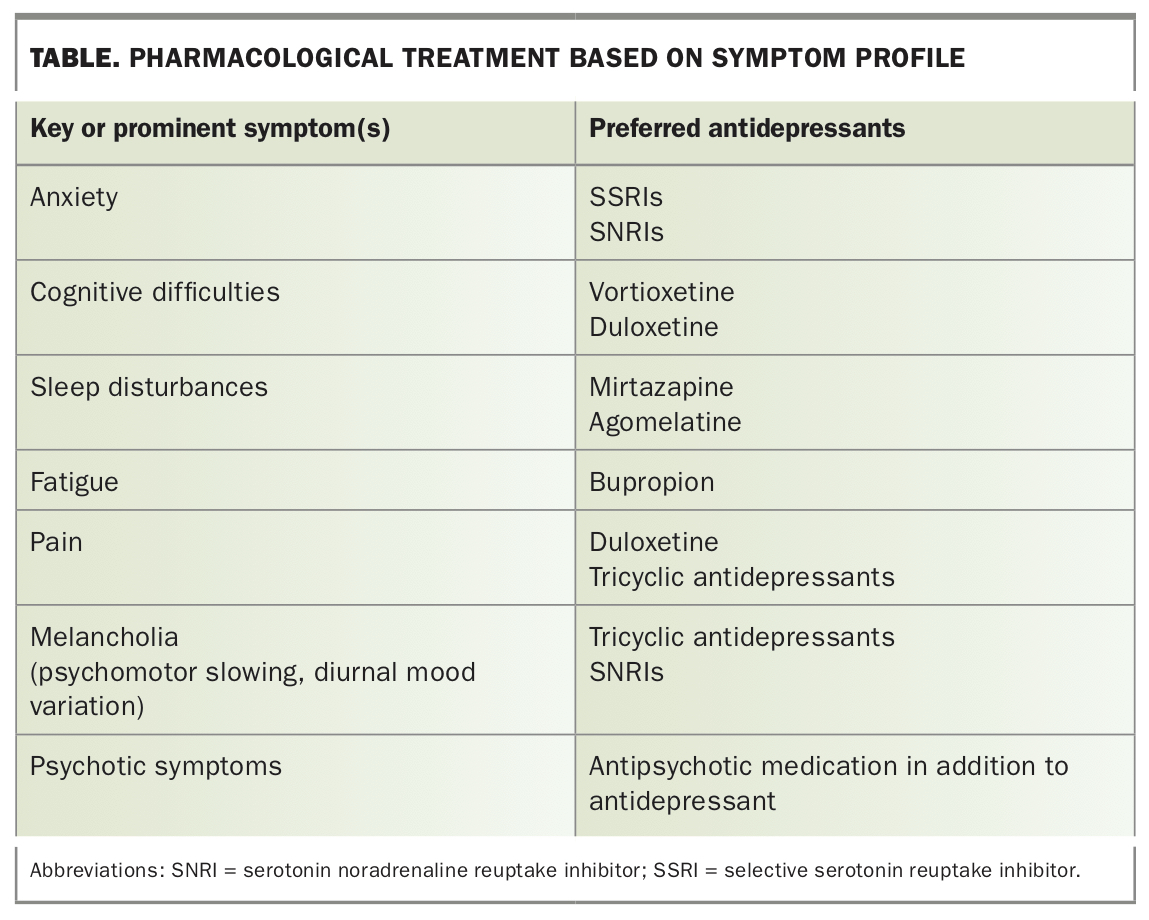
In addition, antidepressants differ in the specific symptoms that they target, and it is possible to choose an antidepressant that matches a patient’s clinical presentation (Table). It is also possible to use the adverse effects to counter specific symptoms. For example, mirtazapine is sedating, so it is sometimes a useful option for patients with significant insomnia. It is also associated with weight gain, which in most cases is undesirable but may be useful for major depression accompanied by significant weight loss. A recent meta-analysis of short-term trials showed the serotonin modulator vortioxetine benefits patients with major depression marked by cognitive deficits.17
{kind=link}
Withdrawal symptoms
Antidepressant withdrawal symptoms have been underestimated, with up to 56% of patients experiencing withdrawal symptoms, and almost half (46%; based on four surveys) regarding their symptoms to be severe according to a recent systematic review.18 These symptoms can persist for months rather than weeks, much longer than previously thought possible.
Patients should be informed about the potential to experience withdrawal symptoms after an antidepressant is commenced for two important reasons. First, if they miss a dose, such symptoms may re-emerge. Second, and perhaps more importantly, they are likely to experience withdrawal symptoms if they abruptly cease the antidepressant of their own volition and should only stop it under medical guidance.
Withdrawal symptoms may emerge after stopping all classes of antidepressants, with the exception of the melatoninergic agent agomelatine, which has minimal, if any, withdrawal symptoms.19 More severe withdrawal symptoms occur with paroxetine and venlafaxine. The risk of withdrawal symptoms is greatest with higher doses and longer duration of use. However, most withdrawal symptoms are usually transient and mild, and resolve with antidepressant reinstatement. Nevertheless, it is important to be familiar with withdrawal symptoms, which are diverse and variably expressed. The acronym FINISH (flu-like symptoms, insomnia, nausea, imbalance, sensory disturbances, hyperarousal) is a useful guide for assessing the domains affected.16,20 Common withdrawal symptoms are listed in Box 4.21,22
{kind=link}
Although all patients are at risk of developing withdrawal symptoms, the risk is greater among patients who have had higher doses than the minimum effective dose of an antidepressant, those who have experienced withdrawal symptoms after missing a dose(s) and those with prior experience of withdrawal symptoms after previously attempting to stop an antidepressant.21,23,24
Strategies for dose reduction
Withdrawal symptoms usually occur after abrupt discontinuation of an antidepressant. Therefore, slowly reducing the antidepressant dose is recommended. There is insufficient evidence to suggest the best regimen for this. A clinical trial found that tapering over two weeks had no benefit over tapering over a few days and, in practice, is still considered a short timeframe.25 Tapering antidepressants down hyperbolically (by lowering the dose by smaller increments over time) in the same manner as benzodiazepines has been recently suggested and is supported by the Dutch Discontinuation of Antidepressants Taskforce.24,26 However, reducing the antidepressant dose in such a way is impractical as current preparations of antidepressant do not allow for the dose to be reduced by such small increments.
For patients with risk factors for severe withdrawal symptoms, the MDcpg2020 recommend initially reducing the dose to the minimal effective dose for two weeks. After this, the dose should be halved, and after a further week, the dose should be reduced more slowly by small amounts (allowing two weeks for each dose reduction), depending on the extent to which the tablet can be divided. Unfortunately, this is not feasible with medications that are encapsulated (e.g. venlafaxine and duloxetine).
An important clinical issue is differentiating withdrawal symptoms from relapse of depression, as the two sets of symptoms have considerable overlap. However, withdrawal symptoms typically start a few days after stopping the anti-depressant and impact different systems. They are not the typical symptoms of a depressive relapse (loss of interest, anhedonia, loss of self-worth or cognitive changes) and usually dissipate quickly after the antidepressant is reintroduced.
Alternative therapies
Pharmacological approaches
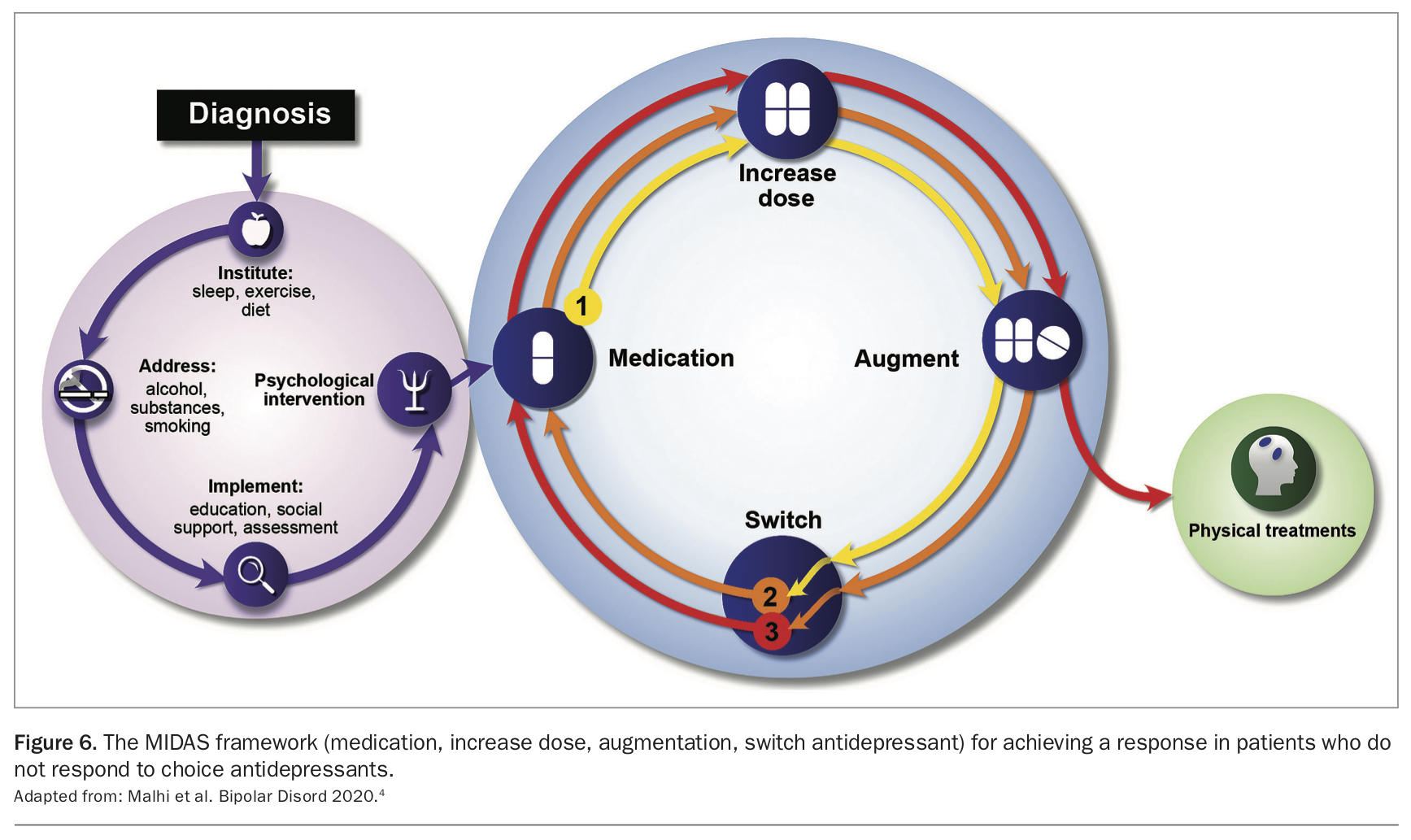
When a patient has an inadequate response to a choice antidepressant, a series of strategies can be implemented to achieve a response, represented by the MIDAS approach (Figure 6). The first step is to start medication (M). If there is inadequate response, increase the dose of the medication (ID). However, increasing the dose to above the highest recommended dose is not recommended as evidence to support this is limited.27
{kind=link}
If there is still only a partial response, or a previous partial response has not been sustained or increased with an increase in dose, augmentation (A) with either a second-generation antipsychotic agent or lithium should be considered. Importantly, augmentation is unlikely to help if there has been no response whatsoever to the primary antidepressant. For the purposes of augmentation, lithium has been shown to be particularly effective in the context of recurrent depression, and prescription of the usual therapeutic dose is appropriate (0.6 to 0.8 mmol/L), although some evidence suggests that even lower doses (0.4 mmol/L) may help.28 The effect of lithium augmentation is likely to be evident relatively soon; it should be withdrawn if no significant improvement is seen within two weeks after a therapeutic level has been achieved. Alternative augmentation agents include the atypical antipsychotics; however, these should not be used long-term because of potential side effects. Again, it is important to note that the augmenting agent is acting on the primary antidepressant prescribed.
If increase in dose and augmentation are ineffective, all medications (anti-depressant and augmenting agent) should be removed, and switching (S) to another medication considered.29 Switching within a class of antidepressants can be effective, as most agents within a class have slightly different specificities of action; however, this should be reserved for intolerability, such as when side effects have precluded an adequate trial of the antidepressant.20 For example, if soon after an SSRI has been prescribed, it has had to be stopped because of an intolerable side effect (e.g. nausea and vomiting), treatment can be switched to another, better tolerated SSRI. However, if the reason for switching is primarily a lack of efficacy, especially after increasing the dose and augmenting, switching to an antidepressant with a different mechanism of action and trialling a molecule from a different class altogether is likely to be more useful.
Ketamine has been used for several years off label for the treatment of depression. Ketamine infusion has a rapid but unsustainable antidepressant effect. Esketamine is the S-enantiomer of ketamine administered by a nasal spray and is approved by the TGA for the treatment of depression for people who have not responded to two adequate courses of antidepressants. It is not yet listed on the PBS and is costly. It needs to be administered at specialty centres, where the patient needs to be observed for 40 minutes after each treatment twice a week. There are no clear indications which patients will preferentially respond to esketamine; therefore, the MDcpg2020 does not make any specific recommendations about its use in depression treatment.
Nonpharmacological approaches
If the patient does not respond to a cycle of the MIDAS strategy, referral to a psychiatrist should be considered for further assessment and alternative treatments. In this context, ECT remains an effective and safe treatment for patients who have not responded to antidepressant medication. However, ECT should also be considered as the initial treatment for patients with severe depression (not eating, severe psychomotor changes or not caring for themselves) or when psychotic symptoms are present. Adjusting electrode placement and pulse width can increase the efficacy of ECT. Unilateral and brief pulse ECT is effective and carries the lowest risk of cognitive side effects. Bilateral and longer pulse width ECT is generally more effective, but has a higher risk of cognitive side effects.
Repetitive transcranial stimulation (rTMS) is a relatively new means of neuro-stimulation. Treatment with rTMS is time consuming (daily treatments for up to 30 sessions) and costly. Although it has some demonstrated efficacy and is generally well tolerated with few side effects, it is not as effective as ECT, and its efficacy compared with other treatments remains to be tested. Further, the type of patients (age, sex, symptom profile) who would benefit from rTMS is not clear.30 For this reason, it remains unclear where to place rTMS among the alternative treatments for non-responsive patients, and there has been significant discussion regarding its optimal use. 30,31 Currently, there is provision for it to attract MBS funding, provided the individual has failed to respond to psychological therapy and at least two different antidepressants.
Conclusion
The MDcpg2020 is a comprehensive guideline providing a framework for the treatment of patients with major depression. This framework covers the required actions that need to be implemented as a foundation for the effective treatment of depression. Included among the actions is the clear recommendation that evidence-based pharmacological treatments should be offered to all patients with major depression. A group of choice antidepressants are identified, based on their efficacy and tolerability. Antidepressants with good tolerability are recommended for use in the first instance. If the patient does not respond to these, medications with greater efficacy (but poorer tolerability) should be used. Antidepressant withdrawal symptoms are a significant problem and patients should be warned about these; a slow reduction of dose (over several weeks) is needed for patients coming off antidepressants. A number of alternative treatments are available to patients who have not responded to choice antidepressants (increasing the dose, augmentation and switching to another antidepressant). Finally, ECT is recommended for those who fail to respond to psychological and pharmacological therapies and for those with a severe depression. MT
COMPETING INTERESTS: Professor Boyce has received research support from the National Health and Medical Research Council, speaker fees from Servier, Janssen and the Australian Medical Forum and educational support from Servier and Lundbeck; and has been a consultant for Servier, served on an advisory board for Lundbeck and as DSMC Chair for Douglas Pharmaceuticals. Professor Malhi has received grant or research support from the National Health and Medical Research Council, Australian Rotary Health, NSW Health, American Foundation for Suicide Prevention, Ramsay Research and Teaching Fund, Elsevier, AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier; and has been a consultant for AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier. Ms Bell: None.
References
disorder: a meta-analysis of three randomized controlled trials. Int J Neuropsychopharmacol 2016; 19: pyw055.
19: 271-780.
J Psychopharmacol 2008; 22: 330-332.
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.